Introduction
L-ascorbic acid (vitamin C) is part of glucose metabolism, which is not accessible to humans since they lack L-gulonolactone oxidase, the last enzyme in the biosynthetic pathway. Therefore, they must obtain it from dietary sources (1). Vitamin C could be found in many fruits such as oranges, grapefruit, strawberries, raspberries, kiwi fruit, and in vegetables such as cabbage, tomatoes, and bell peppers (2). Vitamin C was first isolated by Albert Szent-Gyorgyi in 1928 but the credit for its popularization goes to Linus Pauling. In the 1970s, Pauling implicated the importance of vitamin C in prevention or relief of the simple cold and in the supportive treatment of cancer (3,4). What can be said about vitamin C today, particularly regarding its role in disease prevention and therapy?
Dietary recommendations
The Dietary Reference Intakes (DRI) are the most recent set of dietary recommendations established by the Food and Nutrition Board of the Institute of Medicine, USA, which are based on the evaluation of four categories: Recommended Dietary Allowance (RDA) – the average dietary intake level of a nutrient that prevents a deficiency in 98% of a population, Estimated Average Requirement (EAR) – a nutrient intake value that is estimated to meet the needs of 50% of a population, Adequate Intake (AI) – a value set as a goal for individual intake for nutrients that do not have a RDA, and Tolerable Upper Intake Level (UL) – the highest level of a nutrient that is likely to pose no risk of adverse health effects to 98% of a population. The AI is set instead of an RDA if sufficient scientific evidence is not available to calculate an EAR, such as in infants. The process for setting the RDA depends on being able to set an EAR (5). To provide antioxidant protection, the RDA for adults for vitamin C is set at 75 mg/day for females and 90 mg/day for males. UL for adults is set at 2, 000 mg/day (6). However, many studies have shown that vitamin C intake for optimum reduction of chronic disease risk such as cancer and cardiovascular diseases should be higher than the newest RDA values (7,8). Five servings of fruits and vegetables daily are recomended, because vitamin C as a supplement seems to be less effective in the prevention of diseases and conditions (8).
The role of vitamin C
Vitamin C is an important antioxidant which prevents other compounds from being oxidized. Antioxidative effect of food factors in vivo can be evaluated on the basis of several indices, where vitamin C concentration represents a very sensitive index of oxidative stress (9). It also repairs the tocopheroxyl radical of vitamin E, thereby permitting vitamin E to function again as an antioxidant (10). Vitamin C is a specific electron donor for 8 enzymes involved in collagen, carnitine and noradrenaline biosynthesis, amidation of peptide hormones, and in tyrosine metabolism. It also has non-enzymatic reductive functions in chemical reactions, based on its redox potential and its free-radical intermediate (5). Although vitamin C is a water soluble vitamin which could be easily excretedfrom the body, brain, adrenal cortex, liver, spleen, pancreas and kidney tissues concentrate vitamin C (11). The adrenal gland is among the organs with the highest concentration of vitamin C in the body, where it is required both in catecholamine biosynthesis and adrenal steroidogenesis (12).
Vitamin C metabolism
When given orally, vitamin C is well absorbed at lower doses, but absorption decreases as the dose increases. In the blood, vitamin C is not protein bound, so it is filtered and reabsorbed by kidneys. It probably passes unchanged through glomeruli and undergoes concentration-dependent active tubular reabsorption by a vitamin C transport protein. When the transport protein reaches saturation, remaining vitamin C is not transported, and it is excreted in urine. Vitamin C begins to appear in urine at doses above 100 mg/day (11), while complete plasmasaturation occurs at 1,000 mg/day (8).
Vitamin C is transported across cellular membranes most likely by two distinct mechanisms. Ascorbic acid is easily oxidized to the dehydroascorbic acid (DHA) which is rapidly taken up by cells and reduced to ascorbic acid, using glutathione for reduction (13). Because ascorbate oxidized extracellularly is recycled intracellularly, the process is called “ascorbate recycling”. The specific glucose transporter isoforms, GLUT1 and GLUT3, mediate DHA transport because of its similarity to the molecule of glucose (14). GLUT1 is widely tissue distributed, while GLUT3 is primarily expressed in brain, placenta, testis, and platelets. On the other hand, ascorbic acid is transported into the cell by sodium-dependent vitamin C transporters SVCT1 and SVCT2, one or both of which are found in most tissues (15). Mutant mice SVCT2 have severely reduced tissue levels of ascorbic acid and die soon after birth. The influence of the SVCT2 deficiency on tissue catecholamines is most prominent in the adrenals, where both epinephrine and norepinephrine are decreased over 50% (16). It stillremains unclear which pathways, either SVCT1 and SVCT2 or GLUT1 and GLUT3, dominate in vivo.
Vitamin C has various forms, depending on pH media and its oxidation state (Figure 1). In physiological conditions, 99.95% of vitamin C is present as AscH–, ascorbate monoanion or just “ascorbate” (17).
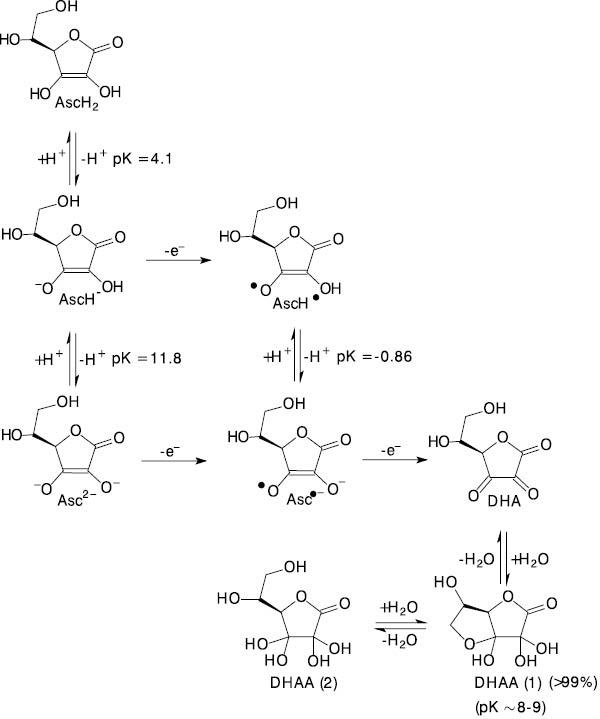
Figure 1. The equilibrium and redox species in the ascorbic acid-dehydroascorbic acid system. AscH2 (ascorbic acid), AscH-(ascorbate monoanion), Asc2- (ascorbate dianion), AscH˙ (ascorbyl radical), Asc·-(ascorbate radical), DHA (dehydroascorbate), DHAA(1) and DHAA(2) (dehydroascorbate hydrolyzed forms) (17).
Interacting with reactive radicals or lipid hydroperoxides, ascorbate releases one electron and a much less reactive ascorbyl radicalis formed. Recently it has been shown that ascorbate can mediate the conversion of hydroperoxy octadecadienoic acids (HPODE) into genotoxic 4-hydroxy-2-nonenal (HNE). However, ascorbate also forms a conjugate with HNE by Michael addition, a two-electron reaction in which ascorbic acid plays the role of a nucleophile. Therefore, vitamin C acts as an electron donor to HPODE, causing HNE formation, and subsequently acts as a detoxifying agent against HNE by functioning as a Michael donor (Figure 2) (18).
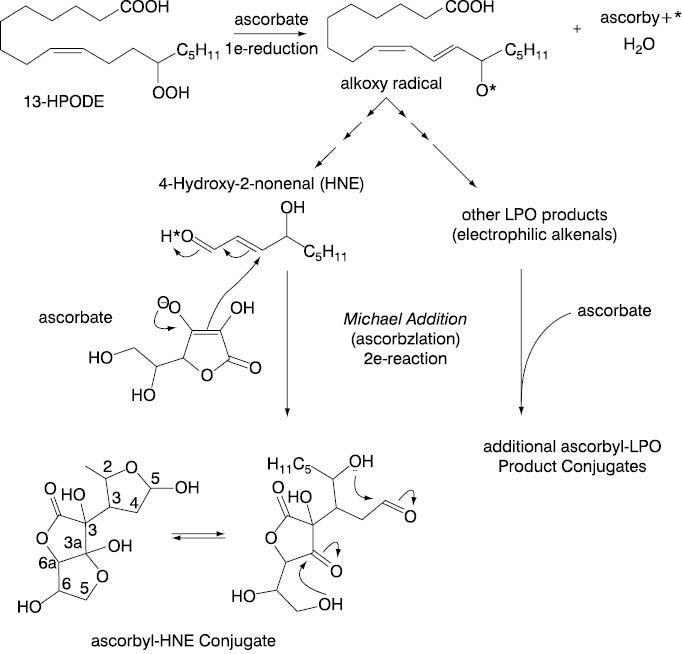
Figure 2. Vitamin C as a one-electron donor and a Michael donor. Vitamin C may function as a one-electron donor to HPODE, thereby inducing formation of the alkoxy radical. The alkoxy radical then undergoes α,β-carbon-carbon bond cleavage, generating HNE as well as other LPO products. Vitamin C may also function as a Michael donor and react with HNE and other LPO products, giving a variety of ascorbyl-LPO product conjugates(18).
On the other hand, ascorbyl radicalundergoes a disproportional reaction, regenerating some ascorbate and producing DHA. DHA is unstable and degradates rapidly in a complex way, eventually producing oxalic and L-threonic acid (Figure 3) (19).
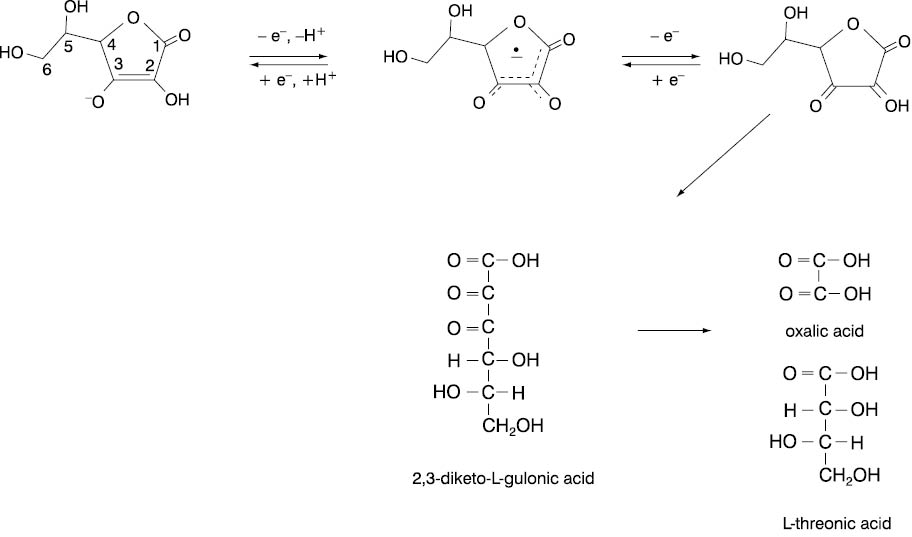
Figure 3. The degradation of ascorbate.
Vitamin C and free radicals
Antioxidant micronutrients, as well as antioxidant enzymes, are the body’s defense systems against free radicals and reactive molecules. The generation of highly reactive oxygen metabolites is a feature of normal cellular metabolism. It is a part of the body’s natural immune system, mitochondrial respiratory chain, arachidonic acid metabolism, ovulation and fertilization. Although free-radical species are continuously produced in the human body, their production can multiply during pathological circumstances (20). Halliwell suggested that the administration of antioxidants can have protective effects or worsen damage, depending on where one is in the sequence of events (21). Administration of a powerful antioxidant after oxidative damage has started could promote damage, and the more powerful the antioxidant is as a reducing agent, the more problems it might cause.
Therefore, it is not a surprise that data related to macromolecular oxidation and high vitamin C intake are inconsistent. They suggest a protective role in DNA oxidation (22,23), but also a pro-oxidant, as well as an antioxidant effect in healthy humans (24). Other data show no effect of high vitamin C intake on either DNA damage or protection against hydrogen peroxide-induced toxicity (25), or efficiency in protecting against chromosome damage (26). On the other hand, a deficiency of vitamin C and some other vitamins and minerals damage DNA by causing single- and double-strand breaks and oxidative lesions (27). Ability of vitamin C to damage DNA, lipids and proteins in vitro is attributed to the formation of reactive oxygen species in the presence of traces of transition metal ions, such as superoxide anion radical and hydrogen peroxide (28):
AscH– + O2 → AscH˙– + O2˙–
AscH– + O2˙– → AscH˙– + H2O2
or even hydroxyl radical (OH·) (29):
Fe(III) + AscH– →Fe(II) + Asc·-
Fe(II) + H2O2 → Fe(III) + OH· + OH-
Hydroxyl radical, one of the most potent free radicals known, can initiate lipid peroxidation, cause DNA strand breaks and oxidize virtually any organic molecule (30,31). Treatment of rats with vitamin C, after chemically induced OH· formation, suppressesthe generation of the radical (32). In healthy volunteers, iron and vitamin C co-supplementation enhanceoxidative DNA damage which is normalized afterwards, perhaps due to adaptations in the cell, such as increase in repair enzyme levels or better sequestration of iron into ferritin (33). However, vitamin C does not further increase the oxidative stress induced by high dietary iron (34). It is noteworthy that iron and copper ions are mainly sequestered in forms unable to catalyse free radical formation. Therefore, their oxidative effect is very limited. Although it still could happen, it is probably masked by the dominant antioxidative effect of vitamin C (20). Indeed, in human plasma taken in vitro, vitamin C acts in the presence of redox-active iron or copper and hydrogen peroxide as an antioxidant which prevents lipid peroxidation and does not promote protein oxidation (35).
Cigarette smoking and vitamin C
Cigarette smokers are known to be exposed to a large number of oxidants (36). Mean levels of vitamin C in the plasma of smokers are twice lower when compared to nonsmokers (37), which increasesthe requirement for vitamin C in smokers. Pretreatment with either vitamin C or vitamin E completely inhibits the DNA damage induced by extracts from cigarette smoke (38). Furthermore, cigarette smoking is associated with endothelial dysfunction including impaired endothelium-dependent flow-mediated dilation (39). The combined usual dosage of vitaminC and E supplements improve the endothelial function in chronic smokers. Also, vitamin C restores impaired coronary flow velocity reserve against oxidative stress in smokers (40).
Vitamin C in disease prevention and therapy
The amounts of vitamin C which safely protect from scurvy may still be too low to provide an efficient rate for other, most likely antioxidant reactions in infected people (41). RDA for vitamin C has health benefit in humans, but higher doses may have the potential therapeutic effects. Clinical studies provide evidence that wound healing in subjects not deficient in vitamin C also can be significantly accelerated with daily dosages of 0.5 to 3 g (42). In cultured human keratinocytes vitamin C acts as a modulator of proliferation and differentiation, directly affecting the keratinocyte or indirectly through effects on fibroblasts (43). Vitamin C modulates the growth and maturation of chondrocytes, and accelerates bone fracture healing (44,45).
Vitamin C participation in immunological defense system has been frequently reported. Phagocytes produce free radicals as a part of the body’s defense against infection, and adequate amounts of a neutralizing antioxidant are required to prevent damage to the immune cells themselves (46). Vitamin C stimulates the phagocytic response of murine peritoneal macrophages (47), as well as the proliferative response of B and T lymphocytes and interleukin-2 and interleukin-6 production in pigs with hereditary deficiency in vitamin C synthesis (48). In humans, combined supplementation with vitamins C and E seems to be even more immunopotentiating than supplementation with either vitamin alone (49).
Decreased blood levels of vitamin C can be found in various diseases. They are associated with, e.g., diabetes mellitus (50), acute pancreatitis (51), asthma (52) or an unstable coronary syndrome (53). Dose concentration studies of vitamin C in healthy people show a sigmoidal relationship between oral dose and plasma and tissue vitamin C concentrations. Therefore, optimal dosing is critical to intervention studies using vitamin C (54).
Common cold
The role of vitamin C supplement in the prevention and treatment of colds remains controversial despite many controlled trials. Studies have shown that high doses of vitamin C taken shortly after onset of a cold did not reduce the duration or severity of cold symptoms in healthy adults (55), but also highly decreased flu and cold symptoms (56). Comparative analysis of thirty trials has shown a modest benefit in reducing duration of cold symptoms from high vitamin C intake (57). The preventive effects of the supplementation seemto be limited mainly to subjects with low dietary vitamin C intake, but therapeutic effects may occur in wider population groups (58). High dose prophylaxis could be notably justified in persons exposed to brief periods of severe physical exercise and/or cold environments. When subjects were under heavy exertion during the trial, like military recruits, the vitamin C protective effect in respiratory infections was highly emphasized (59). Recently, a randomized, controlled 5-year trial suggested that vitamin C supplementation significantly reduces the frequency of the common cold but had no apparent effect on itsduration or severity (60).
Most likely different study conditions provide explanation why so many trials give such contradictory outcomes. Cold symptoms vary diurnally (61), and susceptibility to colds is also increased in smokers, while moderate alcohol consumption is associated with decreased risk in nonsmokers (62). Psychological stress is also associated in a dose-response manner with an increased risk of acute infectious respiratory illness generally (63). It seems that vitamin C produces a greater benefit in cold duration for children than for adults. The dose may also affect the magnitude of the benefit, and there ison average greater benefit from 2 g/day compared to 1 g/day of the vitamin (64). The beneficial effect of vitamin C during a cold probably stemsfrom its antioxidant properties. In an infection, phagocytic leukocytes become activated producing oxidizing compounds that are released from the cells. By reacting with these oxidants, vitamin C may decrease the inflammatory effects that they produce (65).
Asthma and obstructive pulmonary disease
Asthma is primarily an inflammatory diseaseof the airways. Vitamin C plays an essential role in defending against oxidant attack in the airways. Its deficiency in the sputum of asthmatics may be either an underlying factor in the pathophysiology of asthma or a response to asthmatic airway inflammation (65). In exercise-induced asthma, the use of vitamin C supplementation at a dosage of 1 to 2 g per day hasa protective effect in some patients (66). Although studies of vitamin C supplementation suggest a short-term protective effect on airway responsiveness and pulmonary function, a protective effect of vitamin C on the developmentof chronic asthma remains to be established.
Several studies showed a beneficial association between fruit and vegetable intake and lung function (67,68). The forced expiratory volume in 1 second in subjects with the intake of fruits once per week or more was about 80–100 mL higher than in subjects with the intake less than once per week. A 100 mg increase in vitamin C intake per day is also associated with an approximately 10–50 mL increase in forced expiratory volume in 1 second (69).
Cardiovascular disease
Dietary intake of 100 mg/day of vitamin C is associated with reduced incidence of, or mortality from heart diseases, stroke and cancer (7). In elderly people, vitamin C seems to be related to subsequent risk of death from stroke, but not from coronary heart disease (70). Stroke, coronary heart disease, and peripheral vascular diseasehave many risk factors in common, yet somefactors are more important for one cardiovascular disease than another. A high plasma fibrinogenconcentration may be equally importantin all these conditions (71). Increased concentrations of fibrinogen provide a biologically persuasive mechanism by which acute or chronic infection could increase cardiovascular risk. Vitamin C in 2 g/day dose increases fibrinolytic activity and decreases the platelet adhesive index and serum cholesterol (72). Frequent intake of fruit and vegetables, food rich in vitamin C, also increases activity of the fibrinolytic system by lowering plasminogen activator inhibitor activity (73). Seasonal variations in both respiratory infection and cardiovascular disease are attributed to decrease in vitamin C and increase in fibrinogen serum levels during the winter(74).
Total cholesterol, low-density-lipoprotein cholesterol (LDL), and high-density lipoprotein cholesterol (HDL) are among the major risk factors for cardiovascular disease (75). Several studies reported negative correlation between serum vitamin C and total cholesterol (76,77), and positive correlations between serum vitamin C and HDL (78), at least among women (79), but not all studies (80). It seems that vitamin C is involved in cholesterol metabolism in several ways. It reduces 3-hydroxy-3-methylglutaryl coenzyme A reductase activity and cholesterolsynthesis (81,82). It also activates cholesterol-7a-hydroxylase in rats, and the catabolism of cholesterol to bile acids (83).
Intake of antioxidant nutrients may protect against coronary heart disease, because oxidation of lipoproteins is hypothesized to promote atherosclerosis (84,85). It is presumed that oxidized LDL has an atherogenic potential due to lipid peroxidation (86). Ascorbate completely protects plasma lipids against detectable peroxidative damage induced by aqueous peroxyl radicals and it is the only plasma antioxidant that can do so (87). Vitamin C protects against neutrophil-mediated LDL oxidation, most likely due to the scavenging of extracellular oxidants. It also prevents pro-oxidant effects of urate in LDL oxidation (88). Further, vitamin C could help prevent atherosclerosis by strengthening the artery walls through its participation in the synthesis of collagen, and by preventing the undesirable adhesion of white blood cells to damaged arteries (89).
As a powerful antioxidant, vitamin C reverses endothelial dysfunction due to increased oxidative stress, preventing hyperoxic vasoconstriction (90). It also improves lipid-induced impairment of endothelium-dependent vasodilation (91). Experimental studies of essential hypertension suggest that increased production of reactive oxygen species may play a role in the etiology (92). They also show that higher serum levels of vitamin Care consistently and significantly related to lower systolicand diastolic blood pressure among middle-aged or elderly populations (93,94). It has been suggested that 500 mg of vitamin C daily is useful for blood pressure control in patients with hypertension (95). However, in a double-blind, randomized, placebo-controlledcrossover study clinic blood pressure was notreduced after supplementation with 500 mg vitamin C per dayfor 3 months, although daytime levels of ambulatory systolicblood pressure wereslightly reduced (96).
No conclusive evidence is available on the protective effect of vitamin C supplementation on cardiovascular risk, although they implicate a beneficial effect. On the other hand, a diet rich in fruits and vegetables is highly protective against atherosclerosis and coronary heart disease (97,98).
Neurodegenerative disorders
Oxidative stress may play a pronounced role in neurodegenerative diseases. Alzheimer’s disease is the most common cause of dementia associated with aging. It seems that supplementation with antioxidants may delay the development of Alzheimer’s disease. Combination of vitamin E and vitamin C supplements is associated with reduced prevalence and incidence of Alzheimer’s disease (99). Vitamin C and melatonin have beneficial effect on lipid peroxide levels and the activity of antioxidant enzymes in a model of Alzheimer’s disease, suggesting their possible use in the treatment of neurodegenerative diseases (100). Vitamin C also provides protection against scopolamine- and diazepam-induced impairment of memory in mice. The underlying mechanism of memory-restorative action could also be attributed to its antioxidant property (101).
Cancer
Antioxidant and general immunostimulant properties of vitamin C could be beneficial to cancer patients, including tumor regression, and the inhibition of tumor growth. Epidemiological studies show that vitamin C has a protective effect against, in particular, non-hormone-dependent malignancies (102). Experimental in vivo and in vitro studies, however, yielded more controversial results, suggesting that the effects of vitamin C are dose- and perhaps time-dependent with different effects, depending on the species and organ studied or cancer cell type (103).
In the 1970s, Pauling and Cameron used vitamin C in gram quantities in the treatment of patients with advanced stage of cancer. Their results showed improvement of general condition of tested subjects. Most of the patients subjectively felt much better, with reduced pain seizures, and prolonged lifetime (4). Although an experiment performed in Japan yielded similar results (104), a report from the eminent Mayo Clinic showed no effect of vitamin C in cancer treatment (105). However, in the following years researchers revealed a possible role of vitamin C in the cancer prevention. Consumption of foods rich in vitamin C is associated not only with decreased risk of cardiovascular disease, but also of many types of cancer and possibly neurodegenerative diseases. However, the extent to which vitamin C contributes to these effects is still uncertain (106). Reduction in cancer risk is more likely to be achieved through dietary modification, rather than through vitamin supplementation (107). Diets with 200 mg or more of vitamin C per day, obtained from five servings of fruits and vegetables, are associated with lower cancer risk, especially for cancers of the oral cavity, esophagus, stomach, colon and lung. Although several different factors in fruits and vegetables probably act jointly, the epidemiological and biochemical evidence indicates an important role for vitamin C (108).
Supplementation with antioxidants is associated with a decrease in the percentage of cells with chromosome aberrations, andwith beneficial effect in smokers (109). Vitamin C at high concentrations seems to be toxic to cancer cells in vitro (110,111). These concentrations can be achieved in plasma only by intravenous administration. Therefore, negative cancer protective results might originate from the use of oral rather than intravenous vitamin C (11). Following the administration of 1.25 g intravenously, a peak plasma level of 1,000 µmol/L could be reached, although 100 µmol/L could not be exceeded by oral dosing due to limiting absorptive mechanism (112). Most recent data show that, depending on the dose and infusion rate, peak plasma concentrations obtained intravenously can reach 14,000 μmol/L, and concentrations above 2,000 μmol/L may persist for several hours (113). Vitamin C, in concentrations which can be achieved only by intravenous administration, may act as a pro-drug for the formation of hydrogen peroxide, causing death of several studied cancer cell types but no normal cells (114). Diets high in fruit and vegetables, and hence high in vitamin C, have been found to be associated with lower risk for cancers of the oral cavity, esophagus, stomach, colon, and lung (115). Formation of nitrosamines, which is associated with gastric cancer, can be decreased by administration of vitamin C (116). Vitamin C also induces the apoptosis of various cancer cell types by acting as a pro-oxidant and increasing intracellular reactive oxygen species levels (117,118). On the other hand, at lower concentrations vitamin C displays antioxidant property, preventing spontaneous and stress- or antitumor agent-induced apoptosis (116). Furthermore, vitamin C can induce transient cell cycle arrest. Vitamin C inhibits DNA synthesis in HeLa (human cervix adenocarcinoma) cells, delaying the entry of p53-deficient synchronized HeLa and T98G (human glioblastoma multiform) cancer cells into mitosis (119). Fatty acid esters of ascorbic acid have attracted considerable interest as anticancer compounds due to their lipophilic nature which enables their crossing through cell membranes and blood-brain barrier. Ascorbyl stearate inhibits cell proliferation by interfering with cell cycle and induces apoptosis by modulation of insulin-like growth factor 1-receptor expression in T98G and pancreatic cancer cells (120,121).
Current evidence suggests that vitamin C alone may not be effective enough in the treatment of most active cancers. However, vitamin C improves the quality of life and extends longevity in cancer patients, which are the reasons why it should be considered as a supplement in cancer therapy (122).
Diabetes mellitus
Diabetes mellitus is another disease associated with an increased production of reactive oxygen species and a reduction in antioxidant defenses. This leads to oxidative stress, which is partially responsible for diabetic complications (123). Vitamin C status depends on the interactions of dietary intake, plasma insulin concentrations and glycemia. Insulin promotes the active cellular uptake of vitamin C, whereas hyperglycemia inhibits renal vitamin C reabsorption. Oxidative stress is a common pathogenetic factor of diabetic nephropathy. Since DHA and glucose compete for glucose transporters, hyperglycemia discharges vitamin C from tubular epithelial cells, resulting in decreased antioxidant capacity (124). Hyperglycemia and oxidative stress are responsible for endothelial dysfunction in diabetic patients. Intraarterial infusion of vitamin C improves endothelium-dependent vasodilation in patients with either type 1 or type 2 diabetes (125,126). On the other hand, oral high dose of vitamin C could not replenish vitamin C levels and improve endothelial dysfunction (127). Low intracellular levels of vitamin C in individuals with both hyperglycemia and low plasma levels of vitamin C may be responsible for the increasedlevels of DNA damage in such patients. Thus, poorly controlled diabetic subjects might benefit from increased dietary vitamin C (128).
Cataract
Vitamin C, found in high concentrations in the lens, may be of importance for the prevention of cataract in older population (129). Although oxidative damage in the lens can be prevented by vitamin C, a pro-oxidant effect of vitamin C through hydrogen peroxide generation has alsobeen suggested. On the other hand, vitamin C could play a role in protein glycation, which is observed in cataract formation (130,131). In vitro irradiation of aged human lenses with UVA in the presence of vitamin C causes extensive destruction of their chromophores in the UV and visible region, which could be related to glycation products of proteins in lens fiber cells (132). Although mostepidemiological evidence suggests that it is prudent to consume diets high in vitamin C, vitamin E and carotenoids as insurance against the development of cataract (133), it is not yet possible to conclude that antioxidant nutrients have a role in prevention of cataract.
Adverse effects and cautions
Vitamin C supplements are generally well tolerated. However, high doses may cause stomach irritation, nausea, vomiting, drowsiness, headaches or rash2. Adverse reactions are rarely, if ever, seen when the nutrient is consumed according to established guidelines. It should be emphasized that UL values, which are designed to protect the most sensitive individuals in the general population, are not intended to apply to the most sensitive persons in sensitive subpopulations (134). There should be a caution with a highsupplement intake generally, as well as vitamin C, in these individuals. Thus, single 6 g dose of vitamin C induces hemolysis in patients with glucose-6-phosphate dehydrogenase deficiency (135).
Vitamin C has been recognized as the enhancer of the intestinal absorption of dietary inorganic iron, either by reducing it or preventing its chelation by phytates or other food ligands (136). However, it seems unlikely that vitamin C induces iron overabsorption in healthy people (137). Although there has been some concern that people suffering from hemochromatosis (a tendency to iron overload) may be sensitive to high dosages of vitamin C, it seems that vitamin C is entirely safe, even in daily quantities of 10 g or more (138,139).
The contribution of ascorbate to oxalate kidney stone formation is controversial. Since oxalate is a vitamin C catabolitic product, certain concern has beenraised for oxalate excretion. Since gastrointestinal absorption as well as renal tubular reabsorption of vitamin C are saturable processes and the metabolic transformation to oxalate is limited as well, vitamin C should not increase the risk of calcium oxalate kidney stones (140). Thus, an association between high vitamin C intake and increased urinary oxalate excretion(141) or the risk of stone formation (142) has not been found in healthy adults. However, some findings suggested safe vitamin C intake to be less than 1 g daily (8). In some individuals, metabolic conversion of ascorbate to oxalate can cause relative hyperoxaluria and crystalluria, the latter manifesting as hematuria (143). Increased urinary oxalate excretion by intravenous vitamin C administration predisposes susceptible individuals to nephrolithiasis (144). The ingestion of high vitamin C doses should be contraindicated in cases of renal insufficiency, hemodialysed patients, and oxalate stoneformers (145).
Data concerning the effect of vitamin C on urate excretion are also contradictory. Several studies have found elevated urate excretion after prolonged high dietary vitamin C intake (5,146), but not all (147,148). The conflicting findings may be due to lack of steady-state for vitamin C, differences in plasma concentrations, or duration of vitamin C administration. However, in all reports hyperuricosuria was absent at vitamin C doses less than 1 g/day.
High dietary vitamin C intake can also affect certain laboratory diagnostic tests, producing false positive readings in urine glucose tests, protein levels in cerebrospinal fluid and urine, as well as false negative readings in urine bilirubin tests. It also decreases serum bilirubin, cholesterol, creatinine, and triglyceridevalues (145).
Some harmful effects have been mistakenly attributed to vitamin C, including hypoglycemia, rebound scurvy, infertility, mutagenesis, and destruction of vitamin B12 (8).
Interaction with drugs
Drug interactions with vitamin C high doses seem to be very rare. There are some conflicting reports about the effect of vitamin C on decreased anticoagulation response to warfarin or dicoumarol (149). High doses of vitamin C also can reduce steady-state plasma concentrations of indinavir, a protease inhibitor indicated for treatment of the human immunodeficiency virus type 1 (150). On the other hand, vitamin C can improve levodopa absorption in elderly patients with Parkinson disease and with poor levodopa bioavailability (151). High vitamin C intake could also interfere with other drugs, which remains to be established. In addition, diarrhea caused by large oral vitamin C doses can reduce the intestinal absorption generally.
Conclusions
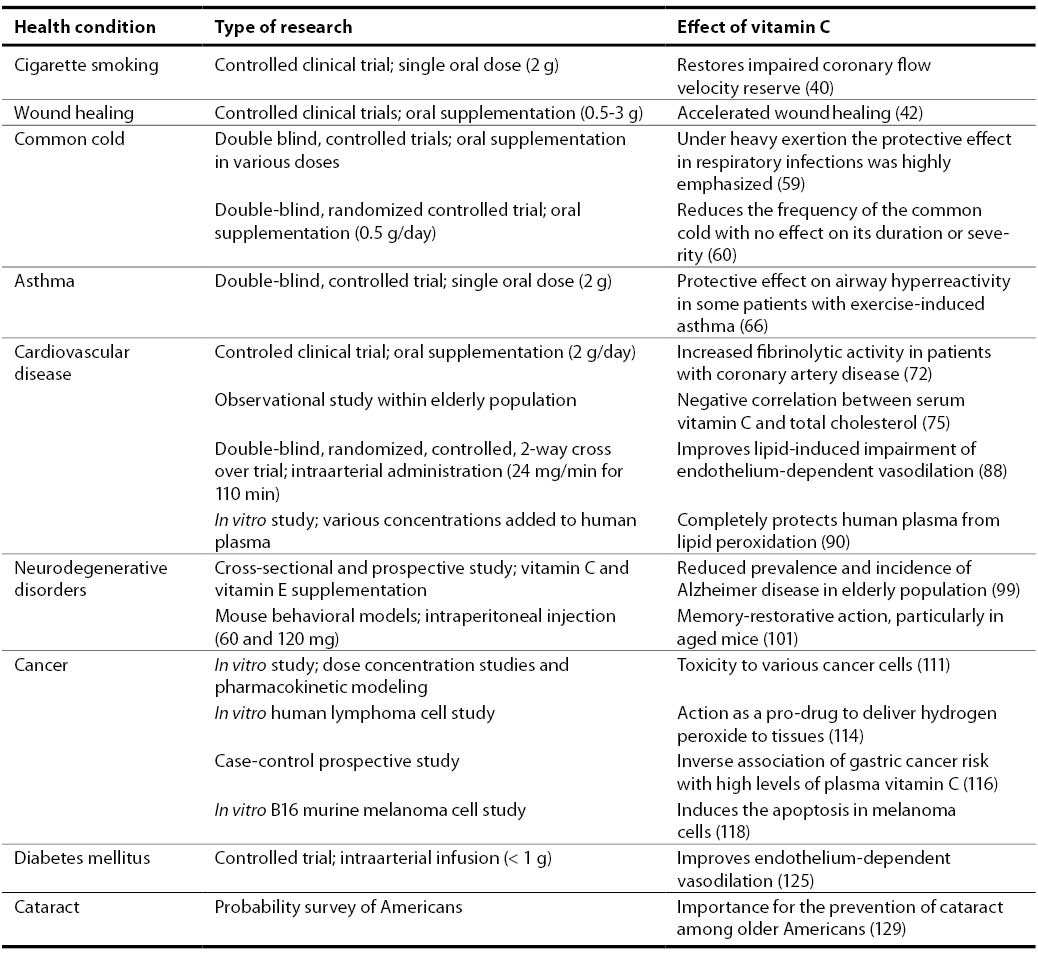
Vitamin C achieves positive results in numerous health conditions, acting primarily as anantioxidant (Table 1). On the basis of current evidence, it is justified to promote diets rich in vitamin C for the prevention against cardiovascular disease and cancer. Vitamin C supplements are beneficial in wound healing, reducing the incidence of common cold primarily in heavily physically stressed persons. It is also effective in preventing plasma lipid peroxidation, and decreasing serum fibrinogen and cholesterol values as risk factors for cardiovascular disease.Howeverer, some positive effects could be achieved only by intraarterial or intravenous administration of vitamin C, such as in patients with diabetes melitus and some types of cancer.The evidence from observational studies also suggests a role of vitamin C in asthma and obstructive pulmonary disease, although causality of the association has not been confirmed. Despite contradictory reports, the consensus from extensive literature is that adverse health effects are not induced in healthy persons by ingesting high doses of vitamin C. However, there should be a caution in persons with some specific metabolic disorders.
Table 1. The effect of vitamin C in various health conditions
Future directions
The evidence in this review provides a substantial basis for further research, both clinical and experimental trials. Oral supplementation of vitamin C cannot yield plasma concentrations as high as parenteral administration. Therefore, further research into vitamin C, particularly as a treatment agent for cancer, as well as clinical study of safety and efficacy of intravenous administration of vitamin C, should be performed to confirm over three decades old Linus Pauling’s idea.