Introduction
Metabolic bone disorder occurs in most patients with chronic kidney failure treated by chronic dialysis primarily due to impaired calcitriol synthesis and increased secretion of parathyroid hormone (PTH) (1,2,3). Other factors, i.e. bone regulatory proteins, have also been implicated, e.g. bone morphogenetic proteins and osteoprotegerin (4). The course of the disease and treatment has an effect on the type of bone turnover disorder, resulting in either high or low bone remodeling (5). High bone turnover is characterized by increased and accelerated bone formation, and high bone resorption rate (6,7). The consequences on the skeletal system are greater osteoid volume, formation of woven bone, increased and intratrabecular resorption leading to osteopenia or osteoporosis with greater fracture risk (8,9). Osteomalacia or adynamic bone are characterised by low bone turnover, i.e. arrested renewal of bone tissue and microfracture repair also resulting in increased fracture risk (9). Duration of kidney failure and dialysis treatment, PTH secretion and its therapeutic control are important determinants of this bone disorder.
After successful kidney transplantation most metabolic disturbances are resolved, but normalization of parathyroid hypersecretion and disorder of bone metabolism may take 2-4 years (2,10,11,12). Increased bone turnover in kidney transplant recipients is related to previous dialysis duration, PTH levels and thetime since transplantation. The main condition is additionally aggravated by immunosuppressives and corticosteroids, the drugs deleterious to skeletal integrity which are administered in the post-transplant period (e.g. 13,14,15,16).
Assessment of the skeletal status and bone disorder in patients on chronic dialysis and kidney transplant recipients is accomplished by measurement of bone mineral density, histologic/histomorphometric analysis of bone biopsy and determination of biochemical bone markers (17). Products of bone cell activities are measured in serum and urine for indicators of bone formation and bone resorption. Investigation of bone markers has mostly shown increased bone turnover in patients on dialysis and also in kidney transplant patients (7,18,19,20). Comparison of bone markers and bone histology indicated that thebone disorder characterized by high bone turnover could be established by bone markers (21,22,23,24,25). In the case of low bone turnover, measurement of normal or decreased levels of bone markers was not found acceptable for diagnosis of this condition. The reports on clinical utility of bone markers in patients on chronic dialysis treatment and kidney transplant recipients differ depending on bone markers measured and patient population characteristics. In order to contribute to the better understanding of metabolicbone disorder, the aim of this studywas analysis of bone formation and bone resorption markers in two separate groups of patients, those on chronic hemodialysis treatment and after kidney transplantation with regard to specific risk factors of this disorder.
Materials and methods
Blood samples were collected in the course of routine monitoring of bone disorder in 79 patients (50 men, 29 women) on chronic hemodialysis and 36 patients (20 men, 16 women) with stable kidney transplant. Bone biopsy was not performed in these patients, but clinical data did not indicate adynamic bone. None of the patients had diabetes. Blood was withdrawn after an overnight fast and before hemodialysis treatment in patients with kidney failure, thesera separated and stored frozen (-20 oC) till assayed within one month of storage. The sera remaining after routine biochemical tests for patient monitoring were used in this investigation.
Hemodialysis patients underwent renal replacement treatment for4 hours 3 times a week, calcium concentration in dialysis fluid was on average 1.50 mmol/L (range 1.25-1.75 mmol/L). Standard therapy for these patients included phosphate binders (calcium carbonate, Sevelamer hydrochloride) and/or calcitriol according to clinical requirements and laboratory tests.
Immunosuppressive therapy in kidney transplant recipients consisted of Cyclosporin A, prednisone and azatioprine mofetil mycophenolate. The mean serum creatinine concentration for this patient group was 119.7 ± 20.5 μmol/L (range 79-168 μmol/L) and creatinine clearance was 70.2 ±13.5 mL/minute (range 51-112 mL/minute).
Data on age, duration of hemodialysis and post-transplant period for the patients comprised in this study are presented in Table 1. No difference existed between sexes regarding age, hemodialysis duration or post-transplant period for each group of patients.
Table 1. Clinical characteristics of the studied patient groups as presented by descriptive statistics (arithmetic mean = X, standard deviation = SD, range).

The following biochemical parameters were measured by commercial kits according to manufacturers’ recommendations: intact PTH (iPTH, IBL, Germany, reference range 1-6 pmol/L; for dialysis patients approximately 3x upper reference limit is recommended), bone alkaline phosphatase (Ostase BAP, IDS, Tyne&Wear, UK, reference limit <22 IU/L) as a bone formation marker, and C-terminal telopeptide of collagen type I (Crosslaps Serum, Nordic Bioscience Diagnostics, Herlev, Denmark, reference limit <0.9 ug/L) as abone resorption marker. In case of different reference ranges for sexes, the values for postmenopausal women were used as the highest result in healthy individuals.
Statistical analyses were performed by a standard statistical package (Microsoft® Office Excell) including descriptive statistics, correlation and regression assessment, student’s t-test (two-tail) for difference between means with significance level p<0.05.
Results
Data on PTH and bone markers showed that no difference existed as tested by t-test between sexes in each of the patient groups. Further statistical analyses were thus carried out for the entire group of patients on hemodialysis or kidney transplant recipients.
Based on the two tail test, patients on chronic hemodialysis were significantly older (p=0.0005) and were significantly longer treated by hemodialysis (p=0.04) as compared to kidney transplant recipients. Differencesin PTH and bone markerlevels were tested by t-test between patient groups (Table 2). Patients on chronic hemodialysis had significantly lower BALP, higher crosslaps and PTH in comparison to kidney transplant recipients (Figure 1). Graphic displays also enable observation of greater ranges for PTH and crosslaps in patients on hemodialysis, while variations are less pronounced in kidney transplant recipients. In a proportion of patients in both patients groups, PTH and bone markers were above the reference range, and percentages of increased results were indicated for each parameter and each patient group in Table 2. For PTH and BALP higher percentages of increased results were found in kidney transplant recipients and for crosslaps in chronic hemodialysis patients. When evaluating PTH results, it should be taken into account that reference limits are different, i.e. approximately 3x higher for chronic dialysis patients.
Table 2. Results of t-test between patients on chronic hemodialysis and kidney transplant recipients. Data are presented as mean and standard deviation, patient population size (n) and percentage of increased values in brackets. Please note that increased PTH for patients on chronic hemodialysis are greater than 18 pmol/L and in kidney transplant recipients greater than 6 pmol/L.
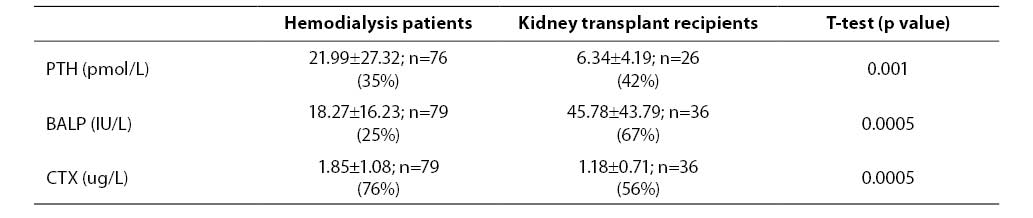
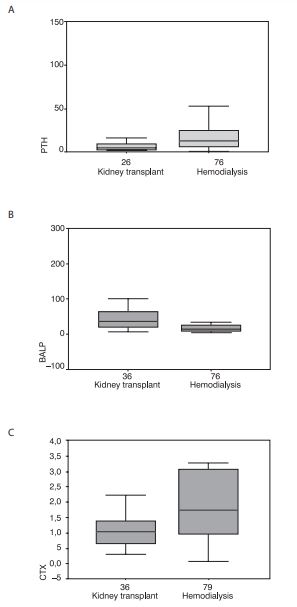
Figure 1. Data on PTH, BALP and crosslaps were significantly different between kidney transplant recipients (kidney transplant) and patients on chronic dialysis treatment (hemodialysis) as presented by box-and-whiskers plots.
Correlations were assessed in order to examine relationships between biochemical parameters and investigated clinical data. In patients on chronic hemodialysis, the duration of hemodialysis treatment correlated significantly and positively with PTH, BALP and crosslaps. Age was found to correlate negatively with crosslaps. Statistically significant and positive correlations existed for PTH with BALP and crosslaps, and BALP with crosslaps. In kidney transplant recipients previous hemodialysis duration correlated significantly and positively with BALP and crosslaps, post-transplant period negatively with crosslaps. Biochemical parameters were also significantly and positively correlated, PTH with BALP, and BALP with crosslaps. Only statistically significant correlations and linear regression equations for pairs significant in both patients groups are presented in Table 3. Figures 2 and 3 show differences in associations of analyzed parameters between the two patient groups. Relationship of BALP with hemodialysis duration demonstrated lesser slope in patients on chronic hemodialysis and a steep increase of BALP with previous hemodialysis duration in kidney transplant recipients. Higher BALP levels in kidney transplant recipients were already reported in Figure 1 and Table 2. Increase of crosslaps in relationship to hemodialysis duration showed a parallel pattern, but higher values in patients on chronic hemodialysis (Figure 2). In relationships of PTH with BALP and crosslaps with BALP, different patterns of associations between patients on chronic hemodialysis and kidney transplant recipients were observed, with steeper slopes for kidney transplant recipients (Figure 3).
Table 3. Statistically significant correlations for pairs of parameters in patients on chronic hemodialysis and kidney transplant recipients presented by correlation coefficient (r) and level of significance (p). Linear regression equations are included only for pairs of variables found to correlate significantly for both patient groups.
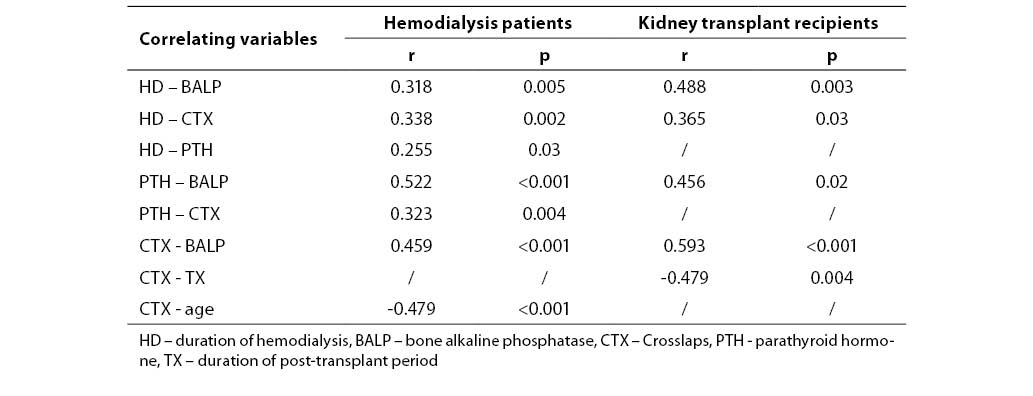
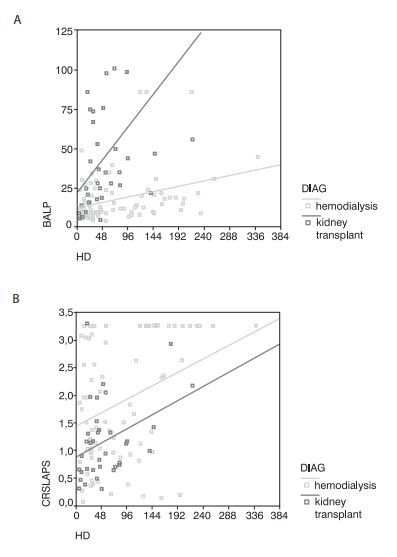
Figure 2. Plots of BALP and crosslaps (CRSLAPS) in relationship to duration of dialysis treatment (HD) for patients on chronic dialysis (hemodialysis) and kidney transplant recipients (kidney transplant) with linear regression indicate different associations of analyzed parameters for patient groups.
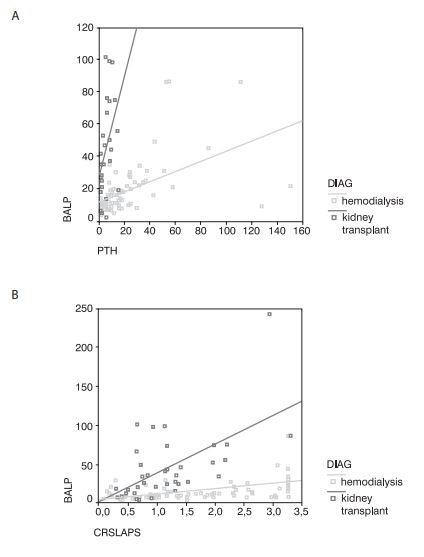
Figure 3. Plots of BALP with PTH and BALP with crosslaps (CRSLAPS) for patients on chronic dialysis (hemodialysis) and kidney transplant recipients (kidney transplant) with linear regression indicate different associations of analyzed parameters for patient groups.
Discussion
In this investigation bone metabolism was compared in patients on chronic hemodialysis treatment and kidney transplant recipients as assessed by PTH and bone markers, and also with regard to age, sex, hemodialysis duration and post-transplant period. Bone turnover was increased in both patient groups, in particular bone resorption. Duration of hemodialysis and PTH were recognized as determinants of increased bone turnover in both groups, and decrease inbone resorption was related to post-transplantation period. In this bone disorder, sex and age were not established as risk factors for impaired bone turnover.
The measured biochemical parameters PTH and crosslaps were significantly higher in patients on chronic hemodialysis in comparison to kidney transplant recipients, and accordingly the percentages of increased crosslaps were higher. The proportion of increased PTH results was lowerin chronic hemodialysis patients, which can be explained by higher reference limit than in subjects with normal renal function (i.e. approximately >3x normal). The fact that increased PTH was found in only 35% of chronic hemodialysis patients also suggested efficient clinical control of PTH secretion. Increased bone turnover in patients on chronic hemodialysis can be explained by the metabolic bone disorder that developed already in the course of deterioration of kidney function (26). The main determinant of accelerated bone turnover is PTH hypersecretion, while increased bone markers are a consequence of both increased, bone cell activity and accumulation of their products due to impaired kidney clearance. An unexpected finding in this study was higher, and in greater percentage increased, bone alkaline phosphatase in kidney transplant recipients than in patients on chronic hemodialysis. This was in contrast with PTH and crosslaps results for the two patient groups. Alkaline phosphatase is not cleared by the kidney and thus not increased in subjects with impaired kidney function. Measurement of bone alkaline phosphatase is thus considered an appropriate marker for assessment of bone metabolism in patients on chronic dialysis (7,27,28). Possible cause of higher BALP in kidney transplant recipients could be the effect of immunosuppressive drugs (cyclosporine A) administered after kidney transplantation which may induce a rise in alkaline phosphatase (29,30). In the early post-transplant period a transient stimulation of bone remodeling was associated to cyclosporine A and decreasing prednisone doses (31). The observed higher BALP values in kidney transplant recipients could be attributed to immunosuppresive therapy but might also be a specific trait of bone metabolism disorder in this patient population. It has beeniswell established that renal osteodystrophy and bone disorder in patients on chronic dialysis and with kidney transplant arecharacterized by great variability in clinical forms, giving rise to a diagnostic and therapeutic problem (17).
Positive association of bone formation and resorption markers in both patient populations indicated the coupling of the bone cell processes in metabolic bone disorder (7,32,33). Differences between the two patient groups in relationships of hemodialysis duration, PTH and crosslaps with BALP were strongly influenced by higher BALP in kidney transplant recipients resulting in greater slope in associations as compared to thedata for patients on hemodialysis.
The correlations found between biochemical parameters and other patient data indicated similarities and differences in characteristics of chronic hemodialysis treatment and post-transplant disorder. Duration of hemodialysis and PTH secretion are determinants of increased bone turnover in patients on chronic hemodialysis treatment and also in kidney transplant recipients (6,20,34,35), as observed insignificant positive correlations in this study. In kidney transplant recipients, previous treatment by hemodialysis correlatedwith the investigated bone markers, but not with PTH. This could be due to moderately increased PTH levels in this patient group, stressing the importance of good control of parathyroid function in the course of the disease (36). In turn, PTH correlated only with BALP, and not with thebone resorption marker crosslaps. Previous hemodialysis duration is a risk factor for increased bone turnover after kidney transplantation, i.e. the pre-transplant bone disorder continues after kidney transplantation (13,14,37). Correlations of hemodialysis duration with crosslaps for both patient groups demonstrated that duration of kidney failure wascorrespondingly detrimental for increased bone resorption (6), which was more pronounced in chronic hemodialysis patients than in kidney transplant recipients. As previously stated, this was primarily due to higher PTH levels found in patients treated by chronic hemodialysis. Similar to patients treated by chronic hemodialysis, PTH level is also an important determinant of increased bone turnover after kidney transplantation (2,13,14). This was not confirmed in this study and was probably a consequence of thespecific patient group and its size. After successful kidney transplantation, bone turnover was normalized in the post-transplant period (13), as observed innegative correlation with bone resorption marker in this investigation and also reported in our previous studies (37,38).
The fact that chronic hemodialysis patients were significantly older and were treated by hemodialysis for longer period than the kidney transplant patient population should not be disregarded. This mostly reflects that patients not fulfilling criteria for transplantation were older and thus longer treated by chronic hemodialysis, which are synergistic factors for disorder of bone metabolism.
Analysis of biochemical parameters in the two patient groups showed no difference between sexes. Bone markers in normal population differ between sexes both in adults and children. The negative influence of female sex on skeletal integrity is also observed in the postmenopause and is recognized as risk factor for osteoporosis. Difference between sexes in patients on chronic hemodialysis or kidney transplant recipients was not found by all investigators (39), thus implying aninvolvement of other risk factors of bone disease as opposed to generally accepted risk factors for osteoporosis.
Most of the relationships between bone markers, PTH and hemodialysis duration are common and similar to patients on chronic hemodialysis and kidney transplant recipients (10). This was reflected in correlation coefficients, which were of identical direction and similar magnitude in both patient groups.
A particular finding for patients on chronic hemodialysis was the negative correlation of age and the bone resorption marker crosslaps. Older age is a risk factor for osteoporosis, although not generally confirmed to be of significance in patients on chronic hemodialysis. In this study, bone resorption was found to be less pronounced in older patients. Similar association was not found for PTH levels.
Measurement of bone markers together with PTH can be considered a useful clinical tool in assessment and follow-up of metabolic bone disorders related tochronic hemodialysis treatment and kidney transplantation (40). It also enables insight into risk factors of this bone disorder and investigation into variations of itsclinical presentations.