Introduction
The development of immunoassays has revolutionized laboratory medicine, especially during the last 30 years. The implementation of new endpoint tracers, new assay formats, automatisation, reproducibility, duration time of assay and availability of analyses have contributed for immunoassays to become everyday practice. The main characteristic of all immunoassays – from immunoprecipitation to biochip assays – is that the reagent that discovers or quantifies the target analyte (antigen) contains the antibody. Despite the specificity of the noncovalent bond between analyte and complementary antibody, numerous interferences (Figure 1) are possible, and can cause false increase (positive interference) (1-3) or false decrease of measured result (negative interference) (4,5). In every research, it is necessary to think about always present predictable and always possible unpredictable and unrecognizable interferences (6). One of the most drastic examples of error in medical practice is the case of false positive chorionic gonadotropin (hCG) test result, described with 22 year old women who underwent, due to unrecognized interference of heterophilic antibodies followed by permanent false positive hCG test result, unnecessary medical interventions: chemotherapy, hysterectomy and segmental lungs resection (7). That case won a lot of public attention (16 million USD damage was paid). Moreover, scientific literature offers similar cases (8,9).
Interferences may be defined as the effect of substances present in an analytical system which causes deviation of the measured value from the true value (10). Some interferences are typical for immunochemical methods (11) The special pre-analytical and analytical interferences have their impacts on the clinical evaluation of immunochemical findings, compared to other chemistry methodologies. Due to the specific features of the immunoassay technique (cross-reactivity of the antibodies, specificity, technology-dependent sensitivity limits, the matrix effect, etc.), which might cause misleading laboratory report.
Manufacturers of reagents for immunoassays are obliged to warn against these interferences, and some of them can usually be found in instructions for analytic procedure. Analyte-dependent interferences relate to interaction of substances present in biological sample and one (1,11-16) or more reagent components (17,18). The interference effect usually depends on concentration of interfering substance (12,19). These analyte-dependent interferences include compounds that are structurally similar with analyte. Therefore, they cross-react with the antibody or other proteins in the sample, e.g. autoanalyte antibodies, heterophile antibodies, human anti-animal antibodies or rheumatoid factors (12). The most frequently described interferences are the ones occurring during hormone determination (5,20-24), tumor markers (25), drugs and metabolites (26-28.), troponin (29-31) and during serological analyses (32,33). Autoanalyte antibodies (autoantibodies) have been described to cause interferences for a number of analytes, e.g. thyroid hormones (total and free forms), thyroglobulin, prolactin (macroprolactinaemia can result in hyperprolactinaemia without pituitary disease), testosterone, insulin (12). Antithyroid autoantibodies have been found in patients with Graves’ disease, Hashimoto’s thyroiditis, hyperthyroidism after treatment, goiter, carcinoma or non-thyroid autoimmune conditions. The presence of rheumatoid factors in serum can cause falsely elevated values in troponin assays as well as in thyroid function methods. Also, paraprotein can interfere in immunoassay by sterical blocking analyte-antibody reaction.
One should suspect interferences in immunoassays upon receiving an unacceptable result, if there is non-linearity during dilution, if there is no agreement with other test results or clinical data, if different immunoassays in determination of the same analyte provide significantly different results. Unawareness and non-recognition of interferences could lead to diagnostic errors, inadequate treatment and monitoring of its efficacy, unnecessary laboratory tests, unnecessary therapy (falsely low analyte concentration can lead to patient overdose). Most of the interferences are typical for all immunoassays (Table 1) and some relate to single methods.
Table 1. Interferences in particular immunoassays
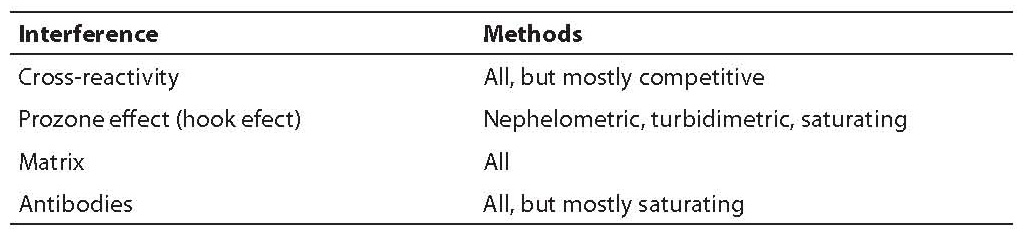
Interfering antibodies can affect all types of immunochemical analyses, but they are most frequently present in saturating analyses. That is because in saturating analyses we have an excess of both antibodies (the capture and the tracer one). Their concentration is higher than the usual analyte concentration and the reaction occurs very fast in conditions of high analytic sensitivity. Any serum antibody having only slight affinity to the capture and the tracer antibody can together with them create a measurable complex. All serum antibodies big enough to bind simultaneously two antibodies from the reagent in the endpoint, provide a measurable signal. One of the common examples of interfering substances are idiotopic antibodies, e.g. rheumatoid factors containing cross-reactive idiotopes (25).
This paper gives a close review of some of the possible interferences typical for immunoassays, especially of those of greater importance for a clinical biochemist: 1) cross-reactivity with endogenous and exogenous non antibody-structured substances; 2) cross-reactivity with endogenous and exogenous antibody-structured substances; 3) the hook effect; and 4) the matrix effect.
Cross-reactivity with endogenous and exogenous non antibody-structured substances
Cross-reactivity is the most common interference in immunoassays, but mostly in competitive ones. It is non-specific influence of substances in a sample that structurally resembles analyte (carries similar or the same epitopes like analyte) and competes for binding site on antibody (34). The interference grade caused by cross-reactivity depends on three factors: antibody specificity, method and sample preparation (35). The most common examples can be seen during determination of hormone concentration, drugs, allergene-specific IgE. Hormones TSH (thyroid-stimulating hormone), LH (luteinizing hormone) and hCG (human chorionic gonadotropin) carry analogue α-chain, and β-chain determines the specificity of the respective hormone – therefore, it is necessary to choose an assay which would be able to recognise different epitopes by using specific antibodies (36). The second example are steroid hormones, which have identical cyclopentanoperhydrophenanthrene structure (37,38). Furthermore, there is prostata specific antigen (PSA) which exists in several forms (total, PSA; free, fPSA; precursor, proPSA and newly also early prostate cancer antigen, EPCA) and causes cross-reactivity and insufficient accuracy (39). Cross-reactivity causes falsely elevated concentration of analyte, but depending on the test method falsely low values can also occur (Figure 1 Ab).
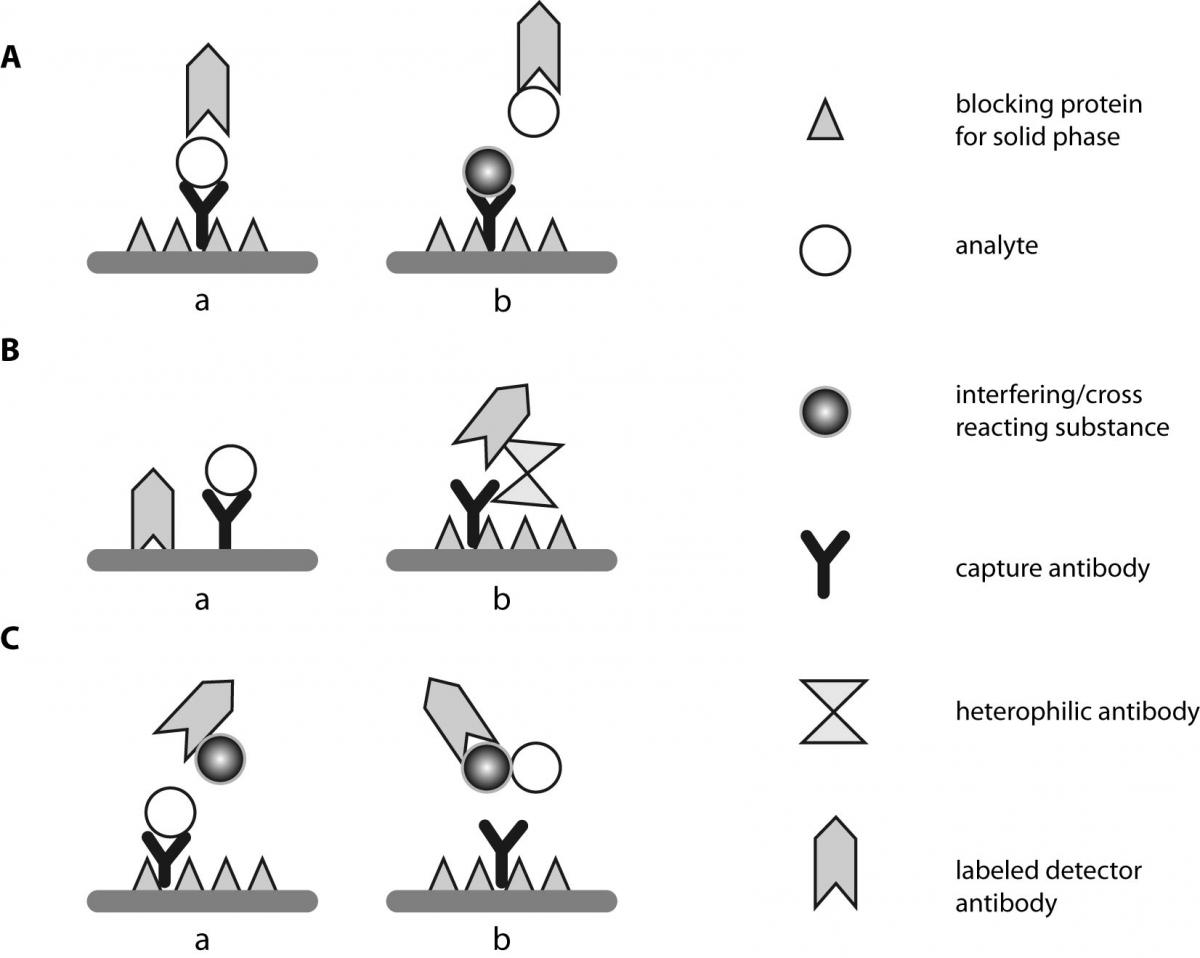
Figure 1. Different interferences in immunoassays: Aa - assay without any interference; Ab - cross-reactivity of an interfering substance with capture antibody, resulting with false negative result; B - positive interference: Ba - unspecific binding of labelled detector (tracer) antibody to a not blocked solid phase; Bb - “bridge” binding by heterophilic antibodies or HAMA, respectively; C - negative interference: Ca - change of sterical conformation after binding of interfering protein to Fc fragment of detector antibody Cb - masking of the epitope on analyte surface by a protein of the sample.
Cross-reactivity can be caused by metabolite or analyte precursor, e.g. conjugated cortisol metabolites by determining the urine cortisol (38) or simultaneous application of medications with similar molecular structure (tricyclic antidepressants) (19). The problem of cross-reactivity by vitamin D (1,25-ŠOHĆ2D3) determination due to possible positive interference of 25-OH D3 (34) is well known. In the area of allergology one can also find interferences (40) by determination of allergene-specific IgE to cow milk (41), mite allergens (42), seafood (43), pollen and latex (44), animal epithelium (45), hymenoptera sting venom allergens (46). Falsely increased concentration of IgE to pollen allergens due to presence of IgE to carbohydrate determinant of the monoglycosylated allergenic molecule have also been reported (47,48). In this case a person despite increased IgE concentration shows no symptoms of an allergic disease. The reason for that is that IgE antibodies to carbohydrate determinants do not affect histamine release from basophilic granulocytes or mast cells.
Cross-reactivity usually causes positive interference, but in some assays negative interference is also possible. So, for example in digoxin-determinating assay oleandrin (digoxin-like cardiac glycoside) can interfere in different ways (49). By decreased digoxin concentrations, oleandrin can have positive interference and by increased concentrations negative interference. In the time of organ transplantations it is important to know that immunoassays for determination of cyclosporine A concentration, an immunosuppressive drug give significantly higher concentration than referent HPLC method (49). Cross-reactivity has also been reported in methods for drug misuse screening (50, 51). Faster dissociation of an interfering substance than of an analyte during washing or separating free from captured analyte during analysis can be the cause for falsely low concentration of an analyte (52).
In competitive immunoassays of small molecules (drugs), both, the capture (binding) and the tracer antibody (labeled detector), bind simultaneously to the analyte. Cross-reactivity is hard to predict, therefore, we must be aware of its existence, be up to date with scientific literature and choose more specific methods.
Cross-reactivity with endogenous and exogenous antibody-structured substances
Immunoreaction can be influenced by antibodies present in biological sample of a patient or antibodies from the reagent (13,53). Biological sample can contain exogenous and endogenous antibodies. Endogenous antibodies are presented in about 40% of patients (14), especially in those who were on immunotherapy with monoclonal antibodies (54). Immunological drugs belong to the group of exogenous antibodies. From this group the most commonly reported interference is the one upon intravenously applied Fab fragment from antidigoxin antibodies (Fab fragment is directed to antigen determinant of digoxin; Fab fragment comes from antidigoxin antibody produced in sheep) (55,56). Interference mechanism of the Fab fragment has different affinity and specificity of capture antibodies in some assays. It has also been reported about interference of ginseng (digoxin-like immunoreactive component) (57).
There are two types of endogenous antibodies in patients’ serum. Heterophilic antibodies (natural antibodies and autoantibodies) (58,59) and anti-animal antibodies (human anti-animal antibodies; HAAAs) (23). Although endogenous antibodies differ in some characteristic (60) they interfere according to identical mechanism in saturating (sandwich) analyses – they simultaneously create complexes with capture and tracer antibodies of the reagent – they “bridge” them (Figure 1). Heterophilic antibodies are multi-specific antibodies synthesised to very poorly defined antigens. Human anti-animal antibodies are antibodies of high avidity and are synthesised to well defined antigens (16).
Heterophilic antibody interference has falsely elevated (Figure 1B) results as a consequence (58,60-64), although falsely low values (31,55,65-67) have been reported in cases when the interfering antibody creates a complex with only one antibody from the reagent. Positive heterophilic antibody interference in sandwich capture assays occurs because heterophilic antibodies “bridge” the capture and the tracer antibody (68). Negative interference occurs due to binding of heterophilic antibodies directly to the capture antibody what disables binding of analytes. In some assays (ELISA, luminometric methods) reagents contain animal proteins (bovine albumin and casein) which block reactive sites on microtiter plates or polystyrenic micro substances. However, their interference ability can go in two directions: they can cause falsely increased results, but also induce increased background signal if the heterophilic antibodies directly bind to them (68). Heterophilic antibodies interfere also during cytokine determination by ELISA (69) whose serum concentration is very low (66,70). Heterophilic antibody interference in cytokine determination can be reduced by adding normal nonimmune animal serum to the sample (68). Interferences in patients with monoclonal gammopathies (69,71) are also possible, as well as interferences in patients with present autoantibodies (31,72).
The most common anti-animal antibodies are human anti-mouse antibodies (HAMA) (14,53,73,74). Mouse monoclonal antibodies are increasingly applied intravenously in diagnostic or therapeutic purposes in oncology (75), allergology (76), autoimmune diseases (77), and some patients synthesise HAMA to them. HAMA can interfere with mouse monoclonal antibodies if they are a component of the reagent. Around 10% of patients carry heterophilic antibodies (12) and around 40% patients who intravenously received mouse monoclonal antibodies will synthesise HAMA. Prevalence of anti-animal antibodies is higher in patients with IgA deficiency (39% carry anti-goat antibodies and 18% carry HAMA) than in patients with normal IgA concentration (22). Some patients can synthesise anti-animal antibodies after exposure to other animal antigens, e.g. in vaccine produced in rabbits or chicken, in anti-snake venom produced in the horse, in professional exposure to pets and other animals (45).
Reagents for saturating analyses usually contain serum or some other blocking agent that should diminish the non-specific interference (20,53,78-81). If interference is expected, it is useful to have an additional blocking agent to treat the samples (78). There is no universal blocking agent for all analytes and all methods. The agent that after validation showed as the best for reducing the effect of heterophilic antibodies for certain analyte must be applied (53).
The hook effect
The hook effect is based on the saturation curve of antibody with antigen (Figure 2). Primarily, the hook effect depends on analyte concentration (34,82-85). It implies the presence of huge excess of analyte which saturates all binding sites on antibody (86-89). The effect occurs mostly (but not exclusively) in assays where all three components (antigen, antibody and marker) incubate simultaneously (single step assay) (90). The hook effect does not occur in competitive immunoassays. That means that in reaction there is a surplus on analytes that did not penetrate to analyte-antibody complex compound. This results in falsely decreased value of the measured analyte which could even lie in the reference interval. The value of absorbance in the post-zone (down-side of the curve) is identical with the absorbance value in the pre-/pro-zone (up-side of the curve). In this case, the reaction curve is bell-shaped (bell-shaped curve) or hooked (34). Some automated analysers have a system for recognizing excess of an analyte while the sample is being simultaneously diluting. The most automated analysers used in clinical chemistry only warn about non-linear reaction what is sufficient to see if the sample needs to be diluted. Manufacturers of reagents for immuno-turbidimetric determinations have reduced the hook effect by introducing latex particles as carriers on which the reaction between analyte (antigen) and antibody takes place. In competitive assays the hook effect was eliminated by introducing a wash step (this wash step is programmed in current automated analysers) upon reaction of analyte with the capture antibody and addition of the tracer antibody (86-90). Reagents manufacturers reduce the hook effect by increasing the quantity of the capture and the tracer antibody and by reducing the quantity of samples required for the analysis.
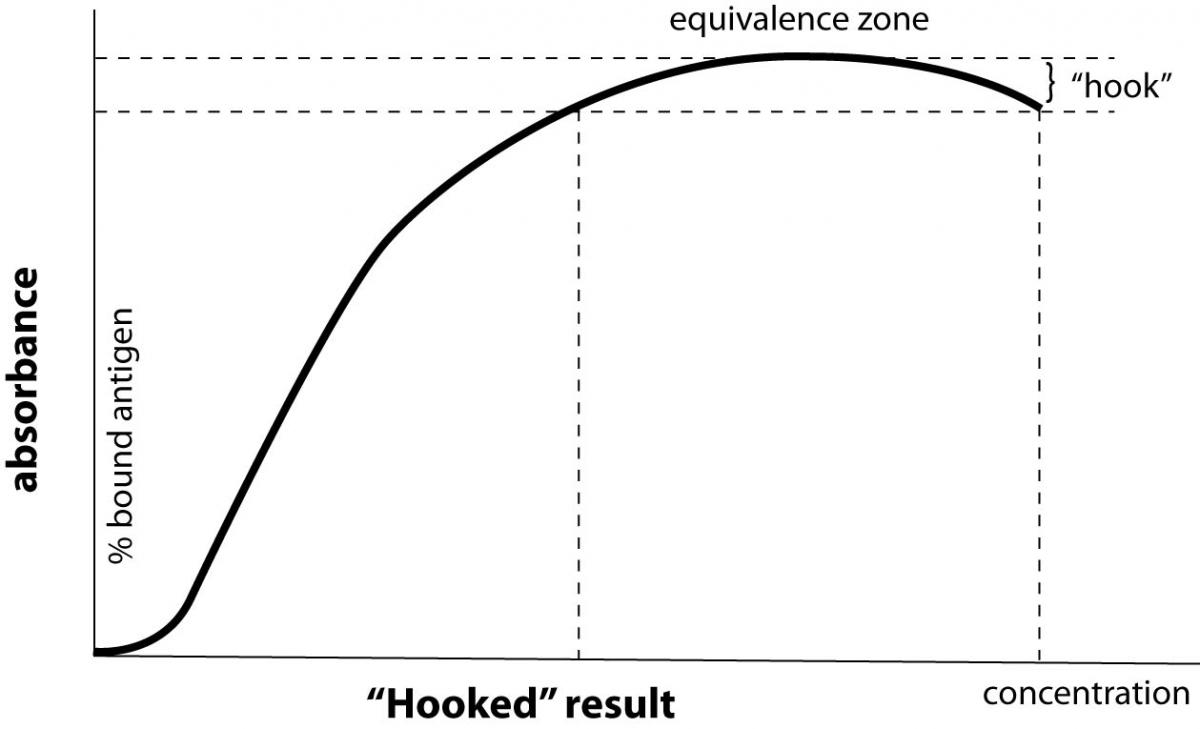
Figure 2. The hook effect - An excessive amount of analyte overwhelms the binding capacity of the capture antibody. This results in an inappropriately low signal that causes erroneous low or normal result (“hooked” result) for a patient with an excessively elevated serum analyte concentration.
The hook effect is common phenomenon in everyday work of a clinical laboratory and on no account should be neglected. It exists by analytes present in serum in extremely wide range of concentrations like C-reactive protein (100-fold increase), antistaphylolysin antibodies (10-fold increase), hormones (at 6-fold concentration increase) (hCG), IgE (>1000-fold), ferritin (100-fold increase), tumor markers (especially CA 19-9, PSA) (34). Tumor marker determination is mostly influenced by possible huge concentration increase (>10,000 fold) that exists in patients with extreme tumor growth. It can occur at the initial laboratory workup of the patient. The cut-off value, where the linearity of turbidimetric methods is lost, is shifted towards higher values by introducing latex particles as antibody carriers. If the reagent manufacturer has not marked the cut-off analyte concentration above which the hook effect occurs, medical biochemist should investigate this and record this data into the manual on work quality of the laboratory. The possibility of the hook effect occurrence is discovered by determining sample with exceptionally high concentration in nondiluted form and in dilutions 1:10 i 1:100 (34,91). If in diluted samples higher values are measured than in nondiluted sample, we are talking about the hook effect. The reliable determination of cut-off concentration follows afterwards. The sample must be diluted until the results of two different dilutions match (taking into consideration the dilution factor). If extreme increased value of the measured analyte is expected, two samples could be prepared – the nondiluted and the diluted one.
The matrix effect
Serum or plasma sample is a complex compound of lipids, proteins, carbohydrates, salt and water. The sum of interferences of all sample components (with exception of analytes), which affect the target analyte to be measured is known as “the matrix effect” (92,93). The most serum components that cause so called matrix effect have low affinity of binding to an analyte or antibody. This component disguises usually the analyte or the antibody causing the absence of the binding reaction of analyte to antibody.
Except of these endogenous elements (94), which cause inter- (25) and intra-individual variability (95-97) of results, the concept of the matrix effect could be widened to exogenous components that relate to the impact of anticoagulant during plasma sampling (98) or the impact of coagulation activator and separator during serum sampling. Heparin therapy in patients with acute myocardial infraction (AMI) affects the result of determination of troponin I concentration (96). Due to negative charge of polyanions heparin binds with cations of troponin (96). This can result either in conformational changes in troponin molecule or in directly covering epitopes involved in the immunoreaction with antibodies from the reagent. Besides, heparin binds with different affinity to some troponin forms present in patient’s blood in different phases after myocardial infraction (95). EDTA can act upon release of free cTnl from calcium ion dependent cTnI-troponin C complex (96) what causes falsely decrease of values in methods containing antibodies, directed to troponin complex. Despite the recommendations that heart markers should be determined in plasma, especially in emergency department (99), the sample of choice for troponin determination is serum, collected in tubes with or without gel or in thrombin tubes with or without gel (95).
Gel used as serum separator can adsorb analyte what can cause falsely lowconcentration of drugs prescribing, e.g. antidepressants, benzodiazepine (100). Five to thirty % of the drugs can be adsorbed on gel and if the sample is kept for longer time (24h) adsorption can rise up to 40%. In case the sample for analysis requires freezing, the serum must be placed into a separate test tube (101). There are several different types of test tubes with gel of different quality available on the market today. Therefore, one should be cautious in choosing them and the need for their validation by determination of some analytes is rising.
The cause for result variability may be in the matrix of the calibrator (102,103) or the control samples (17) due to the fact that their matrix is not identical with the biological sample in which some analyte is being determined.
Conclusion
Today, immunoassays are not applied only in specialist laboratories but also in medical biochemical laboratories (104) and especially in private laboratories. Saturating methods are used for determination of hCG (105), thyroid hormones (20,106), cardiac marker (29-31,107), tumor markers (55,73,74,108,109) and in these analytes it has also been reported about interferences of heterophilic antibodies. Prevalence of interference is lower in analyses used for longer period of time (manufacturers of reagents and analysers tended to eliminate them) than in those which are in use for shorter period of time (110). Special attention must be paid to assays with bedside measurements where is also reported about interference of heterophilic antibodies (111).
Knowledge of numerous interferences is a prerequisite for their recognition which helps avoiding possible undesirable consequences important for the patient (diagnostic errors, treatment and monitoring of its efficacy, unnecessary therapy) and for the health care system as well (unnecessary additional researches).