Introduction
Biostatistics is widely accepted as a powerful tool for understanding and analyzing data and there is a constant increase in the use of statistical methods in scientific biomedical literature. The inappropropriate use of statistical methods is a serious problem and may lead to distorted results, incorrect conclusions and a substantial waste of financial and other resources (1). Moreover, it can have serious clinical consequences and is therefore considered as highly unethical (2,3). Errors may occur due to the lack of competence, honest error or even negligence and deliberate deception (4). Unfortunately, a great number of published medical research contains some statistical errors (5-8).
To prevent or at least reduce the error rate and to improve the quality of their articles, many scientific journals have introduced a statistical peer-reviewing process, or even statistical editor (9,10). Furthermore, many guidelines concerning research methodology, study design, data analysis and reporting, have been published. However, the improvement has been only modest and some major problems with research methodology and statistical analysis still exist in the biomedical literature.
Biochemia Medica is a peer reviewed clinical chemistry journal published since 1991. Its editorial board and policy has gone through a major change in 2006 (11) and journal was soon accepted for indexing in some major biomedical bibliographic databases (12,13), pointing to the constant improvement of the quality of the journal content (14). Since 2006 journal has implemented a statistical review for all manuscripts submitted to the journal for possible publication. To educate and help its readers and potential authors in understanding some basic statistical concepts, journal has in 2006 launched a Lessons in biostatistics section, under which many educational articles have been published so far (15-24).
The aim of this study was to assess the frequency of several most common statistical errors, in manuscripts submitted toBiochemia Medica for possible publication, during the 4 year period, since 2006-2009.
It should be mentioned here that authors were informed about all errors identified by the statistical review, manuscripts were thoroughly revised and almost all errors were corrected prior to publication.
Materials and methods
All original scientific and professional manuscripts submitted to Biochemia Medica during the 2006-2009 were eligible for the study, if they contained some kind of statistical analysis of the data. Manuscripts were reviewed manually by two reviewers. Following errors were included: 1) incorrect use or presentation of descriptive analysis; 2) incorrect choice of the statistical test; 3) incorrect use of statistical test for comparing three or more groups for differences; 4) incorrect presentation of P value; 5) incorrect interpretation of P value; 6) incorrect interpretation of correlation analysis; 7) power analysis not provided. Errors under #2 did not include incorrect use of statistical test for comparing three or more groups for differences.
Statistical analysis
Descriptive data were presented as number and proportions of articles within various categories. Statistical analysis was done using MedCalc ® statistical software (MedCalc 9.3.0.0, Frank Schoonjans, Mariakerke, Belgium).
Results
We identified a total of 55 eligible manuscripts submitted to Biochemia Medica, out of which 18 were subsequently rejected and 37 accepted for publication. None of the eligible manuscripts reported power analysis. As of other 6 errors analyzed, at least one error was observed in 48/55 (0.87) manuscripts. Only 7/55 (0.13) manuscripts had none of the errors analyzed in this study, with the exception of power analysis. The frequency of statistical errors in manuscripts submitted to Biochemia Medica during the studied period is presented in Table 1. Most common errors were incorrect use of statistical test for comparing three or more groups for differences and incorrect presentation of P value.
Table 1. The frequency of statistical errors in manuscripts submitted to Biochemia Medica during 2006-2009. Errors are sorted according to their frequency.
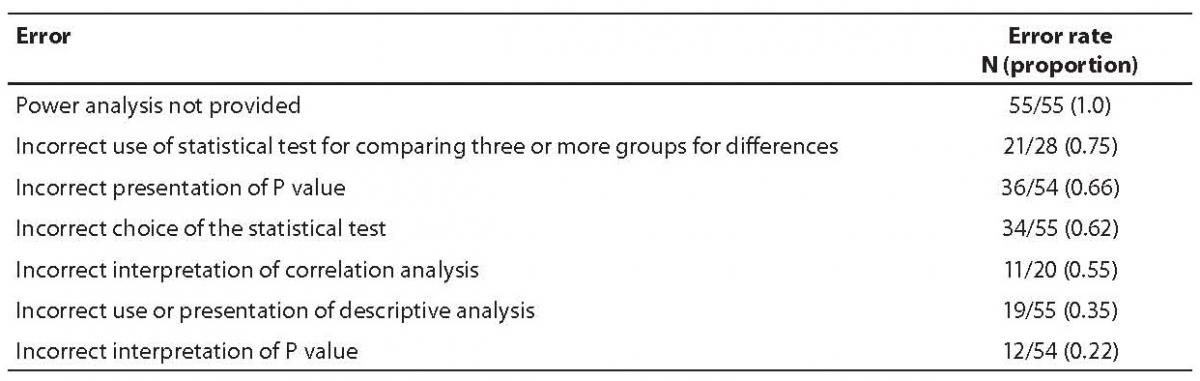
Incorrect choice of the statistical test was present in 34/55 studied manuscripts. Most commonly authors failed to: (i) use non-parametric test like Mann-Whitney Rank Sum test when sample is too small, or when data are not normally distributed instead of using parametric statistical methods (i.e. t-test); (ii) use paired tests when samples are dependent (paired); (iii) use Fisher exact test instead of testing data with chi-square test, due to the low cell frequencies.
As of the incorrect use or presentation of descriptive analysis, errors most often done by authors were: (i) using mean and standard deviation (instead of median and IQR, interquartile range) to describe data sets with non-Gaussian distribution or when samples are small; and (ii) using standard error of the mean (SEM) as a measure of data variability.
Discussion
The phenomenon of inappropriate use and misuse of biostatistical methods is well known and extensively discussed in the literature. Incorrect design of the study and statistical flaws inevitably lead to incorrect conclusions and such shortcomings may be misleading to the clinical practice and waste of the valuable health resources. The aim of this work was to assess the frequency of some most common statistical errors in manuscripts submitted to Biochemia Medica during 2006-2009. Our analysis revealed that a substantial proportion of manuscripts involved at least some statistical error. Power analysis was never provided and most common errors were incorrect use of statistical test and incorrect presentation of P value.
Properly designed experiments should ensure adequate power to detect reasonable departures from the null hypothesis. Power analysis is usually used to calculate the minimum sample size required to some specific analysis. In general, the larger the sample size, the smaller is the sampling error. Sampling error is one of the most commonly occurring mistakes in the scientific biomedical literature. Correct and appropriate sampling procedure is a key prerequisite to the validity of the study. If study groups are not representative for the population, authors should not use inferential statistical techniques, i.e. to make conclusions about the population (20,25). Since all eligible manuscripts in our study were lacking power analysis, there seems to be a lot of space for potential improvement, regarding this issue. Authors should be aware of that fact and try to avoid this mistake. When designing the study authors should always remember to calculate the adequate sample size in order not to do the type II error. Readers should be informed whether the size of the sample was appropriate to detect the effect of interest. It should be noted that power analysis is not necessary for simple exploratory studies reporting preliminary results.
Failure to choose the proper statistical test is also a common statistical mistake (26,27). Authors are often unaware of the assumptions that need to be met when applying some statistical test for data analysis. These assumptions are concerning the data distribution characteristics, scale of measurement, sample size, number of groups and observations and some other. A substantial proportion of manuscripts submitted to Biochemia Medica suffer from this error. Authors are advised to always check for the assumptions of the test, prior to any analysis and to inform the readers why they chose the test, by stating for example: “... ANOVA test was used for comparison of multiple independent groups and non-parametric Kruskal-Wallis test for distributions that were not normal. “ (28).
As of our results, P value was not presented correctly in two thirds of the submitted manuscripts and not interpreted correctly in more than 1/5 manuscripts. This observation is consistent with what has already been published in scientific literature and this issue has been extensively reviewed (29-31). Authors should have in mind that exact P values should be given for all tested differences and rounded on three decimal places (for example P = 0.048 should be written instead of P < 0.05). Expressions like P = NS (non significant), P > 0.05, P < 0.05 should not be used. Also, P should not be reported with too many decimal places, like for example P < 0.00001, unless there are some exceptional reasons for that. Furthermore, authors often make incorrect conclusions based solely on the P value, disregarding the clinical significance of the results. Absolute differences between groups and their respective confidence intervals should be reported whenever possible, as the magnitude of an effect is not suggested by a P-value. Small differences can be statistically significant, but meaningless, if your sample is too large, whereas large differences can be clinically meaningful, but statistically insignificant, if your sample is too small. Results obtained should be always interpreted relevant to their clinical significance, as was for example, reported by Pasalic D. et al.: “... Though statistically significant, differences in plasma cholesterol (P = 0.001), HDL-cholesterol (P < 0.001), apolipoprotein A (P < 0.001) and triacylglycerol (P = 0.002) concentrations between normal, overweight and obese patients were clinically irrelevant. “ (32).
Another common mistake, quite often observed in manuscripts submitted to Biochemia Medica, is the erroneous data presentation. Incorrect use or presentation of descriptive analysis was present in more than one third of the manuscripts assessed in this study. The misuse of SEM was reported by some other as well. Nagele P. and his colleagues have aimed to evaluate the frequency of inappropriate use of the SEM in four leading anaesthesia journals in 2001 and have found that one in four articles (198/860, 23%) published in four anaesthesia journals in 2001 inappropriately used the SEM in descriptive statistics to describe the variability of the study sample (33).
Lastly, the errors in correlation analysis are also very common in the scientific articles (7). Most commonly, following mistakes are made: (i) parametric Pearson test is performed even though test assumptions are not met for the test; (ii) the results (correlation coefficient - r, and its statistical significance P) of the correlation analysis are misinterpreted; (iii) fitted line is extrapolated outside the data set; and (iv) conclusions on causality are made. Conclusions on causality of the observed relationship are not allowed because correlation only represents the association between variables, but not causation (16,34).
More than half of the studied articles in our analysis were having some problem with correlation analysis. Authors should be sure to check the assumptions for the Pearson correlation analysis: i.e. that both variables are numeric, at least one variable is normally distributed, sample is large and there is evidence for linear correlation (as observed from a scatter plot, or by plotting residuals) (35). If those assumptions are not met, Spearman correlation analysis should be performed. Kuo (7) has studied the extrapolation problem in 4 general medical journals with high impact factor (British Medical Journal, Lancet, JAMA, New England Journal of Medicine). He reviewed a total of 37 articles with scatter plot and has observed that 22/37 (59%) of the published articles had some extrapolation problem, 4/37 (11%) had fitted line reaching meaningless value and 3/37 (8%) stated conclusions about the values outside the range of observed data.
This study was not aimed to be a comprehensive analysis of all potential statistical errors occurring in the manuscripts submitted toBiochemia Medica. The choice of errors to be analyzed was arbitrary and solely based on our experience and knowledge about the specificities in the studied manuscripts. As such, we may have missed some errors not included in this study, such as multiple hypothesis testing, erroneous graphical data presentation, missing data, issues in linear regression analysis, outliers data issues and some other. The main goal of this article was primarily to point out some basic errors and pitfalls to the readers of the Journal and all potential authors, thus identifying potential for improvement.
Herein we conclude that the misuse of biostatistics is highly prevalent in manuscripts submitted to Biochemia Medica. All potential errors identified by statistical reviewer during the review process were successfully corrected prior to publication, what has greatly improved the overall quality of the manuscript. Both, authors and editors should be aware of the importance of uses and misuses of statistical analysis. Clinical chemists and all other scientists in biomedicine involved in any kind of statistical analysis of data should perform their work in a professional, competent, and ethical manner (2). Each step forward in educating potential future authors is beneficial to the level of the ethical, professional and competent research practice as well as to the quality of the papers to be submitted.
Acknowledgments
The authors wish to thank to Marijana Miler for her valuable comments to the final version of the manuscript.