Introduction
In interventional cardiology with stent revascularization, which localizes myocardial necrosis and decreases the possibility for ischaemic bias, it is very important to have reliable early biomarkers of myocardial cell injury. As a diagnostic tool, biomarkers could enable appropriate risk stratification for the increasing number of patients admitted to hospital with acute coronary syndrome (ACS) (1). It is accepted that acute myocardial infarction (AMI) refers to the death of cardiac myocytes because of prolonged ischemia that is in contrast to unstable angina (UA)in which the necrosis of cardiomyocytes does not occur (1-3).The routine introduction of cardiac troponins in the laboratory has radically improved the diagnosis of AMI, because only necrotic cardiomyocytes release these proteins into the blood (1,2). Troponins are more specific and sensitive than the traditional cardiac enzymes, such as creatine kinase (CK) and its isoenzyme MB (CK-MB) and myoglobin (4). However, cardiac troponin I (cTnI) can only be detected at least 4–6 h after AMI onset; moreover, its levels do not peak until 12 hours after onset (detected using classical cTnI enzyme linked immunoassays) (5). Consecutive cTnI measurements in combination with the use of reference change value represent a more sensitive tool for AMI detection and allow the evaluation of AMI at low troponin concentrations (6). There is no basic difference between cTnI and cardiac troponin T (cTnT) with respect to their ability to diagnose AMI; differences most frequently arise from variations in inclusion criteria, sampling patterns, or from the use of assays with different diagnostic cut-offs (1). At 2 h after AMI presentation, high-sensitivity cTnT assays are better diagnostic tools than cTnI assays (7). In addition, cTnT assay has a better prognostic ability than a conventional assay (7). However, the cTnT assay probably reflects early cTnT release from an increasingly permeable myocardial cell membrane rather than from a clinically threatening AMI (8). Thus high-sensitivity cTnT assay is probably not suitable for distinguishing AMI from UA.
During the last 20 years, many scientific groups have been searching for diagnostic biomarkers other than troponins that can predict ischemic myocardial injury (3,4,9-17). Of these, interleukin-6, high-sensitivity C-reactive protein and brain natriuretic peptide have been extensively validated and routinely used (1,3). Heart fatty acid-binding protein (H-FABP) (3,4,10-13) and glycogen phosphorylase isoenzyme BB (GPBB) (14-16) belong to a group of novel biomarkers.H-FABP is a 14.5 kDa, small, cytosolicprotein that is abundant in the cytoplasm of cardiomyocytes, but is present in low concentrationsin the blood and in tissues other than the heart (11). It appears inthe blood as early as 1.5 h after AMI onset,peaks at approximately 6 h, and returns to baseline values within 24 h (11). However, its significance for the diagnosis and prognosis of AMI must be verified in future studies before it can be routinely used. Early biomarker studies have shown that GPBB is a very sensitive cardiac biomarker for early myocardial necrotic cell injury, as well as for ischaemia (15,16). GPBB activation in myocardial ischaemia occurs as a result of an increase in glycogen degradation, which releases GPBB into the bloodstream (16). Its possible ability to discriminate myocardial necrosis from ischemia without necrosis is of a major clinical interest (1). However, there is still an emerging need for earlier and sufficiently specific cardiac biomarkers for ACS diagnosis (3,8,14), with ability to distinguish AMI and UA.
The aim of this study was to assess the diagnostic accuracy of H-FABP and GPBB in ruling-in the acute myocardial infarction in patients with acute coronary syndrome, who were admitted to coronary unit within 3 hours after the chest pain.
Materials and methods
Patients
Between January and September 2011, we have enrolled a consecutive series of patients with chest pain in this cross-sectional study. From total number of patient, the patients having chest pain for longer than 3 hours, having chest pain non-suggestive for ACS, patients who died within 24 hours after the admission, patients who were inappropriately sampled or refused to participate in the study were excluded from the further investigation. Inclusion criteria for ACS were based on the European Society of Cardiology (ESC) guidelines on ACS, with patients requiring 2 out of 3 parameters for the diagnosis of AMI (suggestive coronary chest pain, electrocardiogram [ECG] changes, and a positive cTnI value) (1). In patients with suggestive coronary chest pain with duration ≥ 20 minutes and/or ECG changes (new ST elevation at the J-point in two contiguous leads with the cut-off points: ≥ 0.2 mV in men or ≥ 0.15 mV in women in leads V2–V3 and/or ≥ 0.1 mV in other leads, new horizontal or down-sloping ST depression ≥ 0.05 mV in two contiguous leads; and/or T inversion ≥ 0.1 mV in two contiguous leads with prominent R-wave or R/S ratio > 1). AMI was diagnosed by detecting the increase and/or decrease in cTnI values with at least 1 value above the 99th percentile of the upper reference limit (0.2 µg/L) (1). Patients with negative cTnI values were diagnosed as having UA. All ACS patients (AMI and UA), admitted within 3 h from the onset of coronary chest pain to the Coronary Care Unit (CCU) of the Department for Internal medicine, University Hospital Rijeka, were examined further. Exclusion criteria were congenital heart disease, primary cardiomyopathy, pre-excitation syndrome, an implanted pacemaker or cardioverter defibrillator, acute infection, significant renal impairment (estimated glomerular filtration rate [eGF] < 60 mL/min/1.73 m2 or autoimmune diseases, and reproductive period in women. Patients were classified as ‘smokers’ if they had smoked more than 10 cigarettes per day for > 1 year during the last 2 years. Arterial hypertension was diagnosed if blood pressure was > 140/90 mmHg. Hyperlipidaemia was defined as total cholesterol concentration > 5 mmol/L, low-density lipoprotein (LDL) cholesterol levels > 3 mmol/L, very-LDL levels > 1.7 mmol/L, and high-density lipoprotein cholesterol levels of < 1.30 mmol/L for women and < 1.03 mmol/L for men (18). Diabetes mellitus was defined as fasting blood glucose level of > 7.1 mmol/L (19). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s Human Research Committee. All participants provided informed consent before participating in the study.
Methods
Medical examination and patient treatments
During anamnesis and the first medical examination on admission, age, gender, coronary risk factors including current blood pressure, previous heart disease (AMI, percutaneous coronary intervention, or CABG), and pain initiation-to-admission time were examined for each patient. A standard 12-lead ECG was taken on admission and at 12 and 24 h after the onset of the acute coronary event. Patients were followed up in the CCU during the entire investigation. Patients with ACS were treated according to European guidelines, which were relatively similar for all the patients. The treatment regimen included a β-blocking agent, an angiotensin-converting enzyme inhibitor, statin, and acetylsalicylic acid in accordance with the current European Heart Association guidelines (1).
Blood sampling
To estimate cTnI, H-FABP and GPBB concentrations, blood samples were collected from each patient at admission (“0-h” time point) and after 3, 6, 12, and 24 h.To determine GPBB concentrations, 3 mL of peripheral blood was collected at each time point in a heparinised vacutainer (Becton Dickinson, Plymouth, UK). Within 30 min after collection, the samples were centrifuged at 3000 ´ g for 10 min, and plasma was immediately separated and frozen at -20 °C. H-FABP and cTnI concentrations in serum samples were determined by collecting 3 mL of blood at the same time points as those for GPBB quantification. However, these samples were collected in vacutainers without an anticoagulant. Blood samples were left to clot for 30 min before centrifugation at 3000 ´ g for 10 min. cTnI was assessed immediately from the serum; the remaining homogenate was aliquoted and frozen immediately at -20 °C for H-FABP testing. All samples (10/patient) were kept frozen for not more than 6 months before being tested. Repeated freezing and thawing cycles were avoided, and samples were tested by ELISA within 1 hour after thawing without further dilution. An additional blood sample (3 mL) was used to analyse glucose and lipid concentrations at the time of admission.
Determination of biomarkers
First, patients underwent serial testing with a conventional cTnI assay. The concentrations of cTnI in serum samples were analyzed immediately after centrifugation on the Dimension RxL (Siemens Healthcare Diagnostics, Newark, NJ, USA) by using reagents manufactured by the same company (Dimension Clinical Chemistry System, Heterogeneous Immunoassay Module, and Flex Reagent Cartridge). The detection range was between 0.04 and 40.00 ng/mL, with intra-assay coefficient of variation (CV) < 6.85% and inter-assay CV of < 10% and a cut-off value of 0.2 ng/mL (CV < 10%) (20).
H-FABP concentrations were determined by an ELISA test (Hycult Biotechnology, Uden, The Netherlands), with the upper limit of the reference range of 5.0 ng/mL. The detection range was between 0.1 and 25.0 ng/mL (21). The GPBB concentrations were determined using the Diacordon GPBB–ELISA test (Diagenics, Dusseldorf, Germany), with the upper limit of the reference range of 7.0 ng/mL (21,22). According to manufacturer, the detection range was between 3 and 100 ng/mL, with intra-assay CV of < 6.85% and inter-assay imprecision CV of < 10.3 ng/mL. The absorbencies of both, H-FABP- and GPBB-ELISA tests were measured using the Microplate reader MRX (Dynex Technologies, Denkendorf, Germany). All the tests were performed in the Department of Laboratory Diagnostic, University Hospital Rijeka, Rijeka, Croatia. The readers of the tests and reference standards were highly professionally educated persons, who were blind for the results of the other test.
H-FABP concentrations were determined by an ELISA test (Hycult Biotechnology, Uden, The Netherlands), with the upper limit of the reference range of 5.0 ng/mL. The detection range was between 0.1 and 25.0 ng/mL (21). The GPBB concentrations were determined using the Diacordon GPBB–ELISA test (Diagenics, Dusseldorf, Germany), with the upper limit of the reference range of 7.0 ng/mL (21,22). According to manufacturer, the detection range was between 3 and 100 ng/mL, with intra-assay CV of < 6.85% and inter-assay imprecision CV of < 10.3 ng/mL. The absorbencies of both, H-FABP- and GPBB-ELISA tests were measured using the Microplate reader MRX (Dynex Technologies, Denkendorf, Germany). All the tests were performed in the Department of Laboratory Diagnostic, University Hospital Rijeka, Rijeka, Croatia. The readers of the tests and reference standards were highly professionally educated persons, who were blind for the results of the other test.
Statistical analysis
Data analyses were performed using the SPSS 15.0 statistical package for Windows, Version SPSS Inc. 2006. (Chicago, IL, USA). The concentrations of H-FABP, GPBB, and cTnI deviated significantly from normal distributions (P < 0.05) when measured by Kolmogorov–Smirnov tests (part of SPSS 15.0 statistical package) for patients in both the AMI and UA groups in each particular time point tested. Therefore, non-parametric tests were used for further evaluation of data. A non-parametric Mann–Whitney Utest was used to determine the difference between the 2 groups. A P-value of < 0.05 was considered statistically significant. The chi-square test was performed for the categorical variables, with 2-tailed P-values of < 0.05 regarded as significant. Continuous variables were presented as medians and 25th–75th percentiles, and categorical variables were presented as percentages. The receiver operating characteristic (ROC) curves were generated for each enzyme to assess the ability of each biomarker to be used as an early indicator of AMI. The area under the ROC curve (AUC) was calculated with 95% confidence interval (CI). Sensitivities, specificities, positive- and negative-predictive values, positive and negative likelihood ratios, and risk ratios for AMI were calculated for each biomarker to determine its potential to diagnose AMI. Risk ratio was calculated from equation RR = (a / (a+b) / (c / (c+d)), where „a“ represents really positive, „b“ represents falsely positive, „c“ represents falsely negative and „d“ represents really negative. A Z-test was used to compare the sensitivity and specificity of H-FABP with GPBB. Differences in concentrations between the individual markers were tested by Wilcoxon test. A relative increase was expressed as percentage of change from the initial state (0-h time point). The value obtained by the subtraction of 0-h concentration from the concentrations at 3, 6, 12, or 24 h was divided by the value at 0-h time point and then multiplied by 100. The power of study was calculated on the basis of cTnI values obtained in patients with AIM and UA. It accounts 0.845 or 84.5%, what was acceptable, due to desired statistic power > 80%. The power study was calculated using PS Power and Sample size Calculations, Version 3.0, January 2009, according the reference (23).
Results
Patient characteristics
Out of the 214 patients admitted to the CCU with chest pain, 122 patients were excluded from the study after anamnesis and physical examination (Figure 1). Patients who had experienced chest pain for more than 3 h at admission (N = 108) were excluded from the study. Of the patients who experienced chest pain for less than 3 h at the admission, 14 were excluded from the study because of non-suggestive coronary chest pain (N = 7), refusal to participate (N = 1), death within 24 h (N = 3), inappropriate blood sampling (N = 3) (Figure 1). Patients with a suggestive coronary chest pain within less than 3 h before admission (N = 94) were included in the study and cardiac markers were assessed. Patients with outlier concentrations of cardiac biomarkers (N = 2) were also excluded from the study.
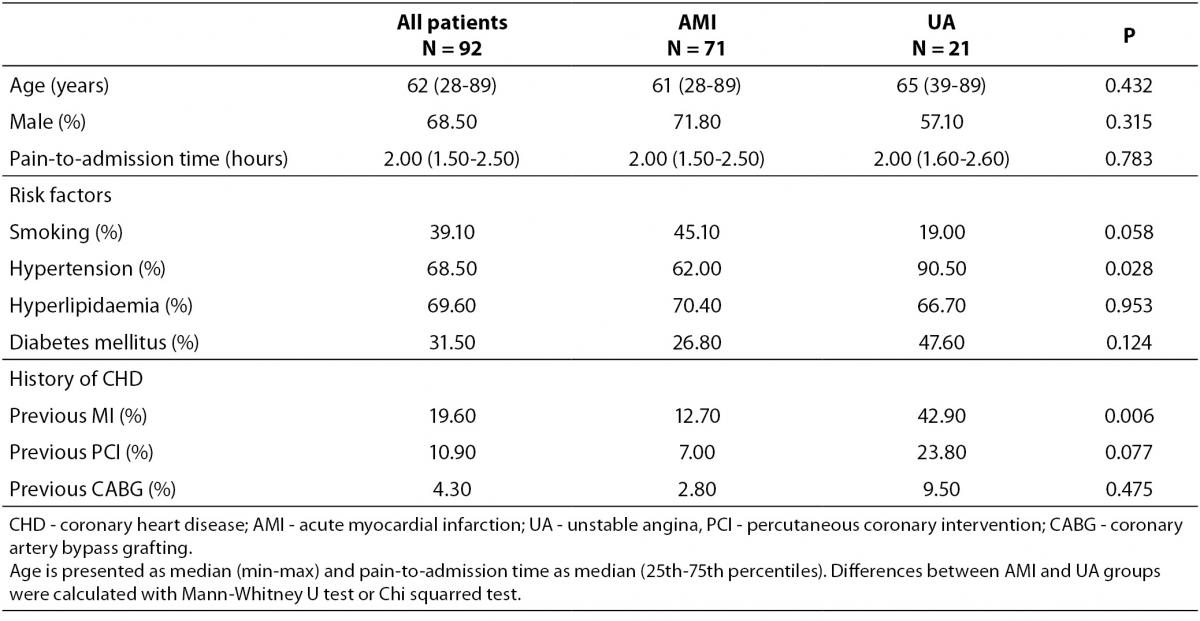
The median time from symptom onset to presentation was 2 (1.5-2.5) hours for AMI group and 2 (1.6-2.6) hours for UA group (Table 1). Patients were divided into 2 groups on admission: patients with AMI and positive cTnI level (N = 71) and patients with UA and negative cTnI level (N = 21), which were determined from ECGs and cTnI concentrations (Figure 1). Beside cTnI, in both groups H-FABP and GPBB were assessed at the admission.
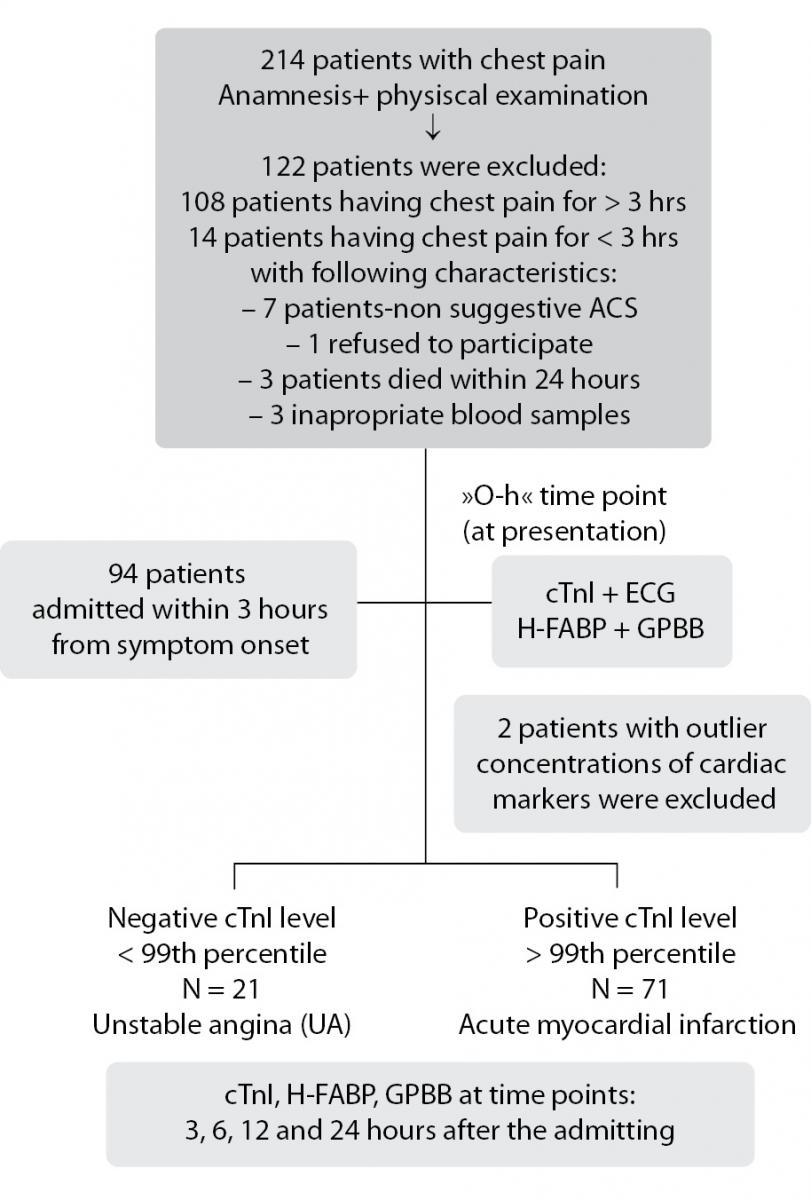
Figure 1. Recruitment of patients presenting with chest pain and results of early measurement of cTnI.
The groups did not significantly differ in age, sex and pain-to-admission time (Table 1). In the group of UA, hypertension was found in 90.5% of patients, what was significantly higher when compared to the AMI group (62%, P = 0.028), whereas other risk factors such as smoking status, hyperlipidemia and diabetes mellitus did not differ significantly (Table 1). Previous myocardial infarction was more common in patients with UA then in patients with AMI (42.90% vs. 12.70%; P = 0.006), whereas both groups of patients had similar percentage of percutaneous coronary intervention or coronary artery bypass grafting (Table 1).
Table 1. Characteristics of the whole group of patients enrolled in the study and the particular characteristics of patients with acute myocardial infarction and patients with unstable angina.
Cardiac biomarker dynamics
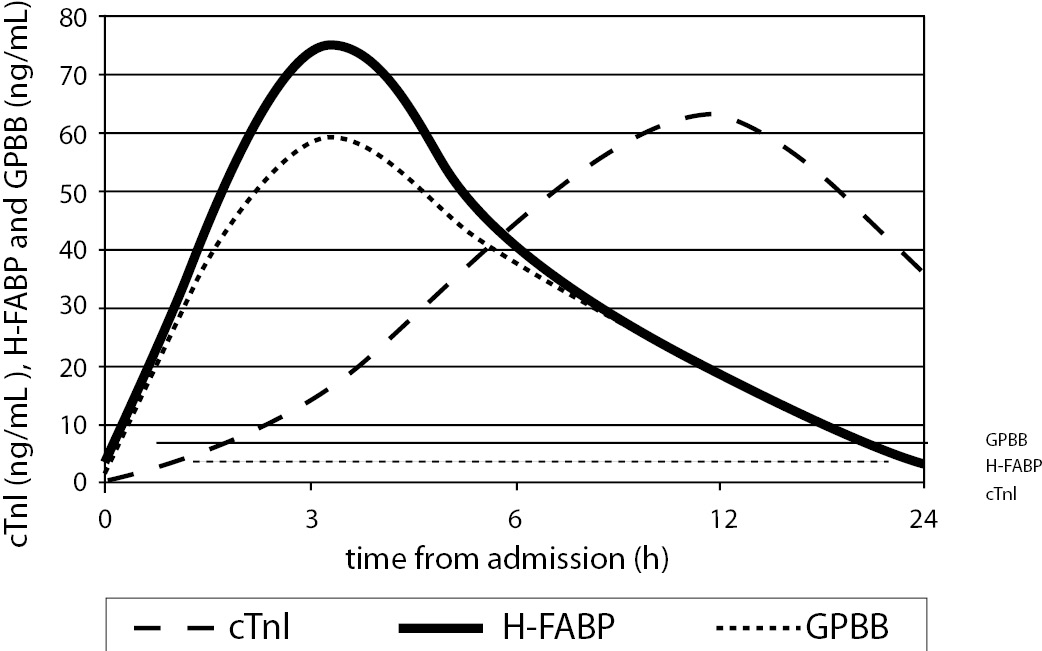
Figure 2 shows cardiac biomarkers concentration dynamics and their interaction during the first 24 h after admission in patients with AMI. At the 0-h time point (within 3 h from the onset of AMI), the concentrations of H-FABP and GPBB were similar and relatively low (P (a) = 0.254, Figure 2A and Figure 2, Table B); however, the levels of both biomarkers were higher than those of cTnI (P (b) and (c) = 0.001, Figure 2, Table B). In the Figure 2, Table B the level of statistical differences (P) between H-FABP and GPBB are designated as (a); between H-FABP and cTnI are designated as (b) and between GPBB and cTnI are designated as (c). Shortly after admission, the concentrations of H-FABP and GPBB rapidly increased to equal levels, peaking at 3 h (73.54 (38.18–110.99) and 58.30 (30.20–122.50) ng/mL, respectively) (P (a) = 0.788, Figure 1A and Figure 2, Table B). In contrast, the increase in cTnI concentration was slow during the same time period; at 3 h, the cTnI levels were lower than those of H-FABP and GPBB (P (b) and (c) = 0.001, Figure 2A and Figure 2, Table B). However, rapid increase in cTnI concentrations was prominent at 6–12 h after admission, which was accompanied by a corresponding decrease in H-FABP and GPBB concentrations (Figure 2A). It resulted in significantly lower concentrations of both, H-FABP and GPBB when compared with cTnI at 6 h (P (b) = 0.003 and P (c) = 0.008) and at 12 h after admission (P (b) and (c) = 0.001, Figure 2, Table B). The H-FABP and GPBB concentrations did not differ significantly between themselves at 6 h (P (a) = 0.97) and at 12h (P (a) = 0.630). At the 24-h time point, the concentration of cTnI was higher than those of H-FABP and GPBB (P (b) and (c) < 0.001), and H-FABP did not significantly differ from GPBB (P (a) = 0.306, Figure 2, Table B).
A
B
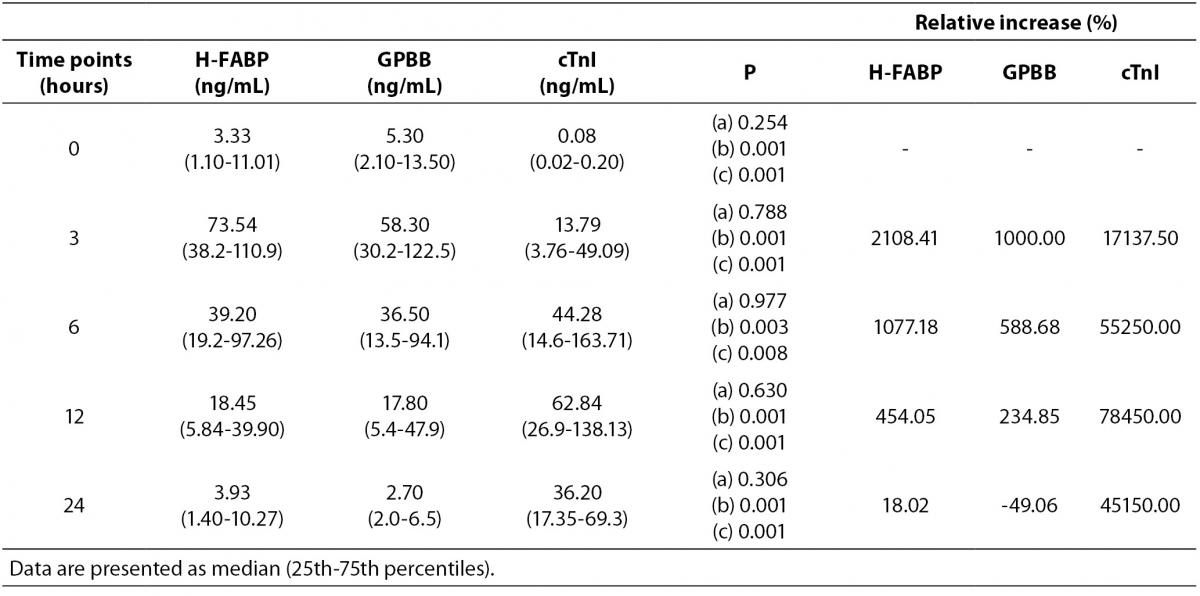
Figure 2. Average dynamics of H-FABP, GPBB and cTnI in patients with AMI (N = 71) admitted within 3 hours from symptom onset is shown graphically (A) and in the table (B). The statistical differences (P values) between H-FABP and GPBB (a); H-FABP and cTnI (b); GPBB and cTnI (c) are calculated with Wilcoxon test.
Table 2. Average dynamics of H-FABP, GPBB and cTnI in patients with UA (N = 21) admitted within 3 hours from symptom onset.
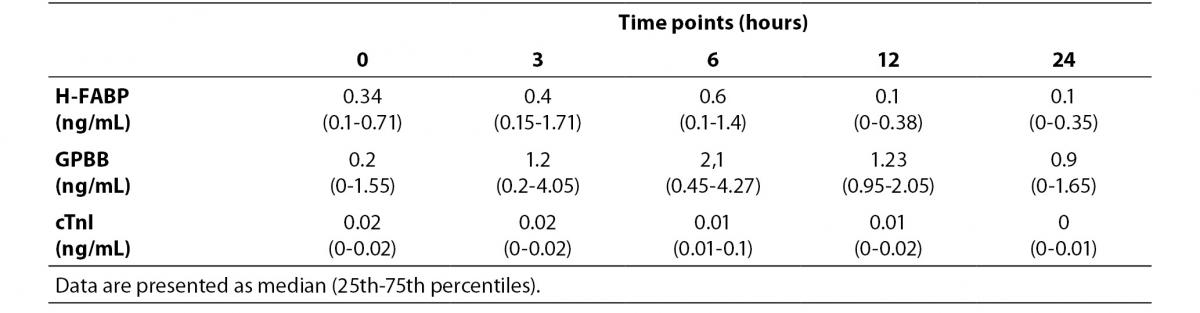
Table 3. Area under receiver operating characteristic curves (AUC) for cardiac biomarkers at the optimal cut off points (99thpercentile of the general population) for the diagnosis AMI in patients admitted within 3 hours from symptom onset (N =71) in respect to patients with unstable angina (N = 21).
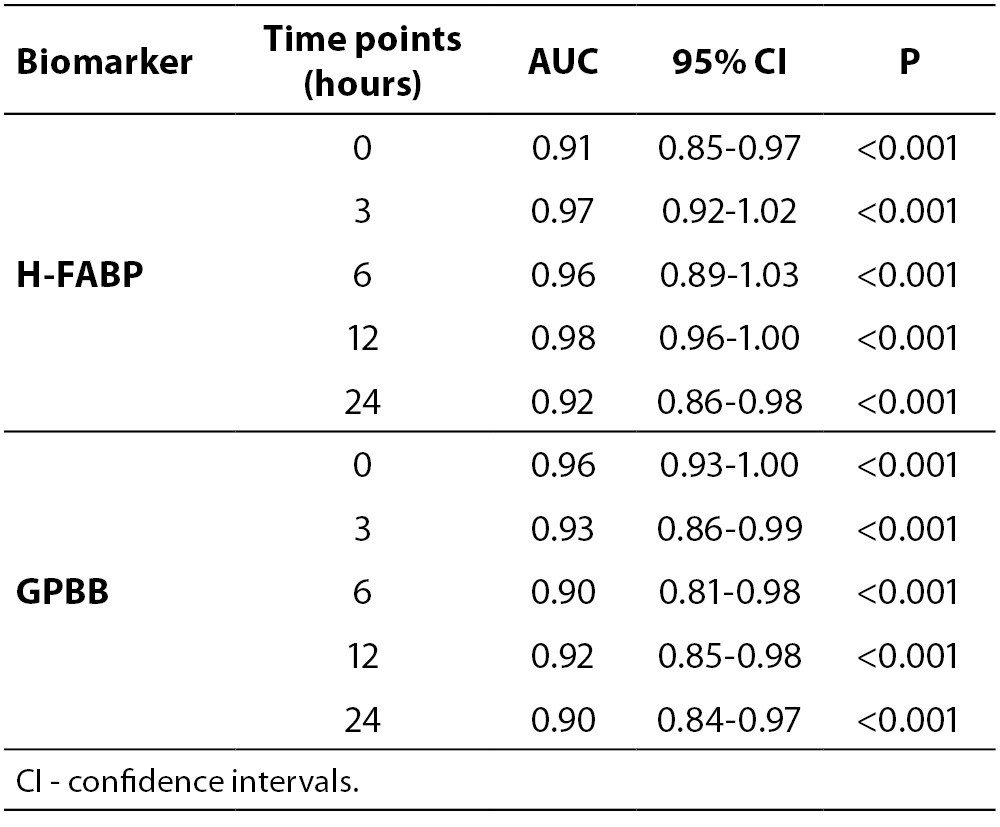
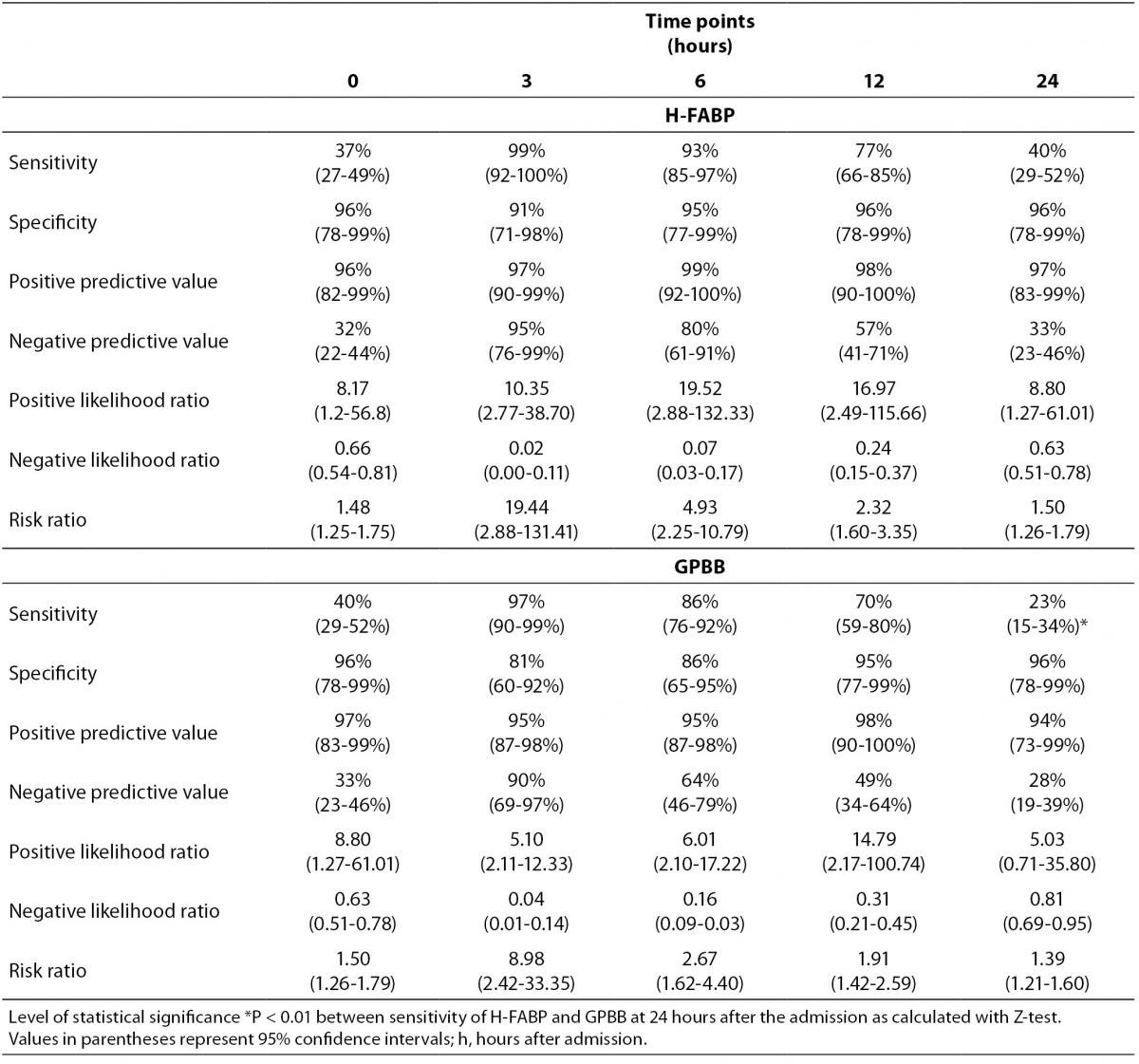
Table 4. Significance of diagnostic H-FABP and GPBB estimation in patients with AMI admitted within 3 hours from symptom onset (N = 71).
Relative increase in H-FABP in patients with AMI is particularly high at 3 h after admission and accounts for 2108.41% from the 0-h time point (Figure 2, Table B). It decreased approximately 2 times at 6 h after admission and again doubly reduced at 12 h after admission (Figure 2, Table B). GPBB followed very similar dynamic, but the relative increase in GPBB was 1000% at 3 h after admission (Figure 2, Table B). At 3 h after admission relative increase in cTnI was 17137.50%, it increased slowly, peaked at 12 h time point, when the relative increase was 78450.00%. After that it slowly decreased at 24 h after admission.The concentrations of H-FABP, GPBB and cTnI in patients with UA were always bellow their cut offs of 5.0 ng/mL, 7.0 ng/mL or 0.2 ng/mL, respectively (Table 2).
Receiver operating characteristic curves
Table 2 shows the AUC for H-FABP and GPBB for the diagnosis of AMI. At admission, for patients having coronary chest pain for < 3 h, the AUC was significantly greater for initial H-FABP (0.91; 95% CI = 0.85–0.97 and GPBB (0.96; 95% CI = 0.93–1.00 in patients with AMI than in patients with UA (P < 0.001); this remained highly discriminatory for all the time points tested (3, 6, 12, and 24 h) (Table 2). There appeared to be no difference between the H-FABP and GPBB ROC curves.
Diagnostic performance of H-FABP and GPBB
In AMI patients, the sensitivities of H-FABP and GPBB at admission were rather low (37% and 40%, respectively) didn’t differ significantly (Table 4). The sensitivity of H-FABP increased at 3 and 6 h after admission (99% and 93%, respectively), which was statistically similar to the sensitivity of GPBB. At the 24-h time point, the sensitivity of H-FABP decreased to 40%; however, this was approximately 2-times higher than the value for GPBB (P < 0.01) (Table 4). The specificity, positive- and negative-predictive values, positive and negative likelihood ratios, and risk ratios for AMI were calculated for both biomarkers (Table 3). The overall diagnostic accuracy of H-FABP and GPBB did not differ significantly.
Discussion
The ability to distinguish acute ACS patients from a very large proportion of patients with cardiac pain is a diagnostic challenge, especially for patients with no clear symptoms, unclear ECG features, and/or borderline diagnostic cTnI concentrations (1). Elderly women who have survived a myocardial infarction frequently visit their doctors complaining of chest pain and have significantly higher mortality rate, target lesion reoclussion (3,24), postinfarction refractory anaemia in the short term, and AMI in the long term (25,26). Although cardiac troponin is a pivotal marker of cardiac ischaemic injury/necrosis (27), a single negative cTnI test is not sufficient to disregard the presence of AMI because of its low sensitivity in the first 3 h of chest pain onset (2,3). Our results showing a slow, early increase in cTnI concentrations to above the cut-off value at the time of early patient admission also suggest this. Therefore, repeated measurements of cTnI concentrations in the period of its higher sensitivity (84.1%) and specificity (93.4%) (28) are required, which comprises the subsequent 6–9 h after admission (27,28). Accordingly, we noticed a rapid increase in cTnI concentrations between 6 and 12 h after admission. This substantially prolongs the time required for an accurate diagnosis after the acute coronary event and reduces the likelihood of achieving high-quality myocardial revascularization by primary percutaneous intervention or stent implantation (25,29). Recently introduced high-sensitivity troponin assays are capable of identifying high-risk patients early and more effectively, providing a reliable and rapid prognosis prediction that enables a fast-track rule-out protocol (3 h) (1,7). However, higher-sensitivity cardiac troponin assays rather reflect the troponin release after increased permeability of the myocardial cell membrane without specifically pointing out necrosis, which is a characteristic feature of a clinically threatening AMI (8). Although cTnT concentrations, measured using high-sensitivity assays, are elevated early after the acute coronary event, its diagnostic accuracy may be compromised because levels can also be elevated in many patients with stable angina (30,31) and in healthy individuals (32), thus weakening its ability to differentiate between healthy subjects and patients with AMI, UA, and stable angina. According to the sensitivity of the ELISAs used in our study, both H-FABP and GPBB markers were not elevated in the patients with UA, which is in contrast to that in patients with AMI, and statistically significant differences were obtained from AUC analysis at all time points tested.This emphasizes the significance of H-FABP and GPBB in distinguishing UA from AMI, particularly during early ACS with peak sensitivities and specificities occurring at 3 h after admission. This is in contrast to other studies, which suggest that H-FABP might be a marker for myocardial ischaemia even in the absence of necrosis (10). Recently, H-FABP has been proposed to be an early marker for ACS because it is only elevated in AMI patients (4,10,17) and appears before the traditional marker troponin in 22% patients at presentation (3). Wiswanathan et al. (10) confirmed the prognostic value and independent prediction of death by using elevated H-FABP levels in low- and intermediate-risk patients with suspected ACS. We advocate the use of H-FABP alone or in combination with high-sensitivity troponin assays to improve the sensitivity of early AMI diagnosis. This is in agreement with the opinion of McCann et al. who declared that assessment ofH-FABP within the first 4 h of symptom onset is even superior to cTnT for the detection of AMI (14). Our results show that GPBB has very similar average dynamics to H-FABP, as reported previously (15). GPBB does not compete with cTnT in terms of sensitivity in AMI patients (14), especially at the first hour after admission (33). Its activation in myocardial ischaemia is a result of an increased glycogen degradation, which results in GPBB release into the bloodstream (15,22) and diminishes its diagnostic accuracy to distinguish between AMI and UA (33). However, its specificity is high and comparable to that of CK-MB (15). All humoral biomarkers have been criticized in terms of their specificity. Accordingly, troponin concentrations may be increased in patients with serious vascular chest pain, non-coronary myocardial injury, skeletal myopathies, or chronic renal failure, resulting in incorrect prognosis (1,8). H-FABP was also criticized for insufficient specificity, owing to its presence in different tissues such as the skeletal muscles, liver, adipose tissue, gut, skin, kidney, or brain (14). The specificity of H-FABP can be improved using modern assays with no cross-reactivity (12) and particularly in combination with high-sensitivity cTnT assay. GPBB isoforms are present in the brain, muscle, and liver, with approximately 80% similarity between the muscle and liver (15). The brain isoform is substantially different and can be distinguished with an appropriate sensitive immunoassay method (15). However, the magnitude of fluctuation, depending on the initial concentration and clinical symptoms, is increasingly important to differentiate between acute or chronic myocardial damage, which has been reported recently for cTnI (6); however, the levels from baseline are still debated (1,2). The results presented in this study show statistically significant changes in the concentrations of H-FABP and GPBB as compared to their initial values (relative increase) at 3 h after the admission of AMI patients. This highlights the importance of H-FABP and GPBB for the early diagnosis of AMI. However, the sensitivities of H-FABP and GPBB in patients with AMI were relatively low at admission (approximately 40% for both markers), similarly to that showed during the first hours after admission (33). However, they concomitantly increased, peaking at 3 h, before gradually decreasing by 20–40% at 24 h. This emphasizes the rapidly changing dynamics of H-FABP and GPBB, owing to the narrow time period of their peak concentrations, relative increases and sensitivities, which highlights the importance of analyzing their concentrations throughout the first 24 h of AMI onset. At 24 h, the sensitivity of GPBB was almost twice lower that of H-FABP, according the results shown herewith. Furthermore, GPBB has approximately twice lower relative increase then H-FABP during the first 24 hours after admission in patients having coronary chest pain for < 3 h, what one should keep in mind during the diagnosis of AMI. In our opinion there is no major benefit to the simultaneous use of H-FABP and GPBB because of their quite similar diagnostic accuracy up to the 24-h time point and because of the cost of such combined diagnostic approach.
In conclusion, our results show that H-FABP and GPBB can improve the early detection of AMI, with a high diagnostic accuracy.These biomarkers are especially useful for distinguishing between AMI and UA within 3 h after admission in patients with chest pain for < 3 hours, which is the time period during which an emergency physician should plan an objective cardiac ischaemia evaluation and appropriate therapy.
Acknowledgements
This work was supported by the grant of Croatian Ministry of Science No. 062-1081875-0545.